BPC-157 — Deep Dive
Category: Peptide / Tissue Repair / Gut-Brain Axis
Full name: Body Protection Compound 157 / Pentadecapeptide BPC-157
Sequence: Gly-Glu-Pro-Pro-Pro-Gly-Lys-Pro-Ala-Asp-Asp-Ala-Gly-Leu-Val (15 amino acids)
CAS: 137525-51-0
Origin: Isolated from human gastric juice
The Unexpected Starting Point
BPC-157 is a synthetic analogue of a peptide fragment found in human gastric juice. Your stomach has been making a version of this molecule your entire life. The body's most corrosive environment — pH 1–2 — is where this compound was discovered, which explains the most non-obvious thing about it: it survives oral ingestion intact.
Most therapeutic peptides are destroyed within minutes in stomach acid. BPC-157 is stable in gastric fluid at pH 1.2 for over 24 hours. It was not designed to resist digestion. It evolved there.
This origin also explains the scope of effects, which looks implausible until you understand the mechanism.
One Mechanism That Explains Everything
Healthy Alfred (@HealthyAlfred):
"BPC-157 has a 100% hit rate across every tissue tested. Severed nerves — regrew. Torn ligaments — rebuilt. Punctured cornea — sealed. Destroyed liver — reversed. Crushed spinal cord — recovery at 360 days."
This sounds like marketing. It is actually mechanistically coherent — once you understand what BPC-157 does.
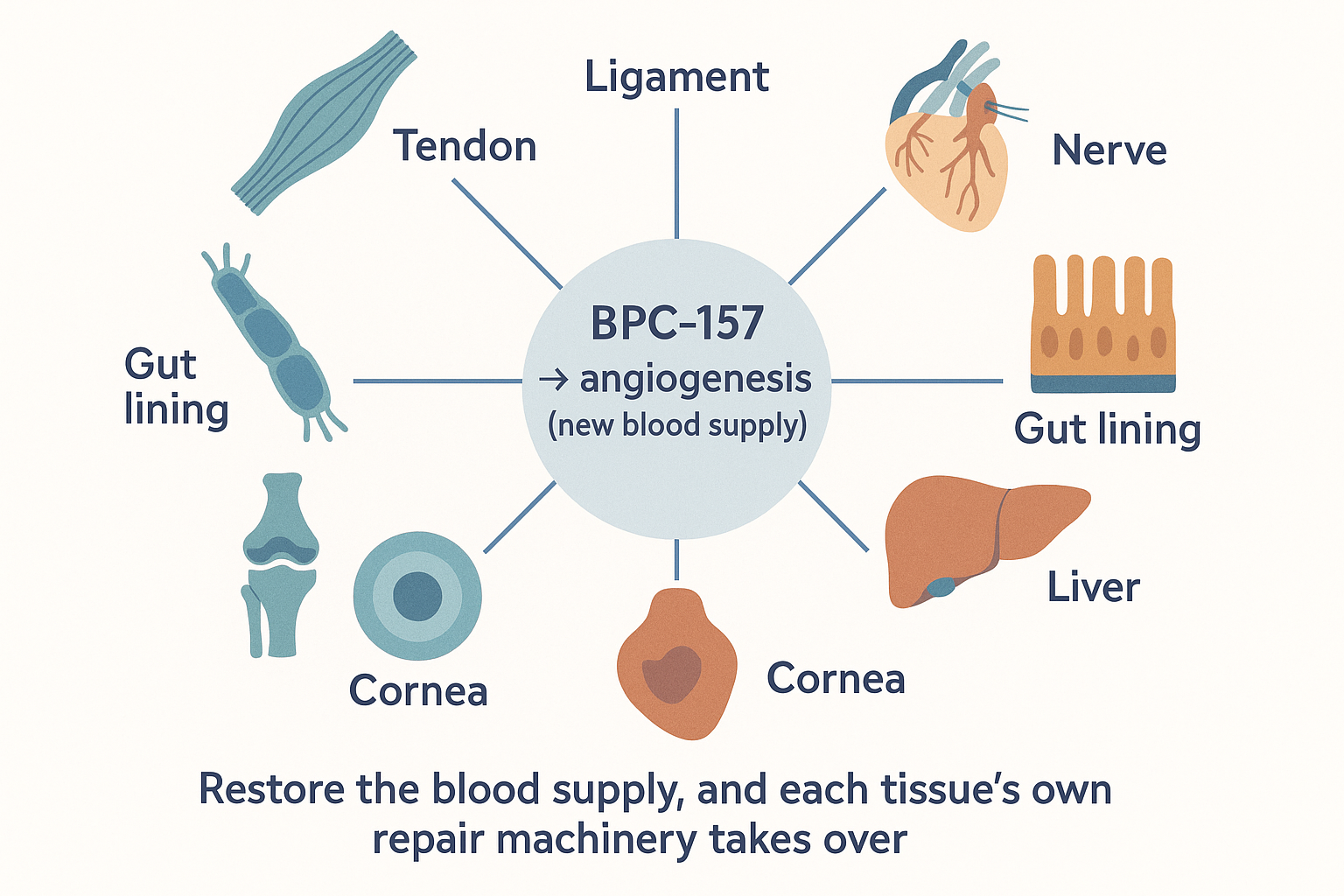 One mechanism, many tissues: BPC-157 restores blood supply (angiogenesis), and each tissue's own repair machinery does the rest — which is why the effect list spans nerve, tendon, gut, bone, and liver alike.
One mechanism, many tissues: BPC-157 restores blood supply (angiogenesis), and each tissue's own repair machinery does the rest — which is why the effect list spans nerve, tendon, gut, bone, and liver alike.
It does not repair tissue directly. It triggers angiogenesis — the growth of new blood vessels into damaged tissue — and modulates nitric oxide (NO) production bidirectionally. Blood supply is the universal prerequisite for repair in every tissue type. Every healing process listed above — nerve, tendon, gut, bone, liver — requires vascularisation. Fix the blood supply and the body's endogenous repair machinery takes over.
The Angiogenesis Cascade
BPC-157 activates two distinct pathways to NO production simultaneously:
flowchart LR
BPC((BPC-157)) -->|"VEGF-dependent"| P1["VEGFR2 ↑ → PI3K → Akt → eNOS"]
BPC -->|"VEGF-independent"| P2["Src → Caveolin-1 → eNOS released"]
P1 --> NO[Nitric Oxide]
P2 --> NO
NO --> ANGIO["Vasodilation + new capillaries<br/>= angiogenesis into damaged tissue"]
ANGIO --> REPAIR["Blood supply restored<br/>→ the body's own repair proceeds"]The dual-pathway redundancy is why even tissues with disrupted VEGF signalling (chronic wounds, scar) still respond.
Nitric oxide then drives vasodilation, endothelial cell migration, and new capillary formation into the damaged area. The dual-pathway redundancy means even tissues with disrupted VEGF signalling (as occurs in chronic wounds and scar tissue) respond to BPC-157.
FAK-Paxillin — Organised Repair Over Scarring
Beyond angiogenesis, BPC-157 phosphorylates focal adhesion kinase (FAK) and paxillin — driving cell migration to injury sites and regulating how collagen is laid down during repair. This is the difference between organised extracellular matrix (functional repair) and disorganised scar tissue (fibrosis). In tendon studies specifically, BPC-157-treated tissue shows organised collagen fibre alignment versus disordered scar formation in controls.
BasedBiohacker (@BasedBiohacker):
"It promotes organised collagen deposition instead of scar tissue — better function and appearance post-injury."
Note: FAK phosphorylation is also one of the two mechanistic vectors behind the theoretical cancer concern (see Safety section below — PMID 12838315).
GH Receptor Sensitisation — Not a Secretagogue
BPC-157 upregulates growth hormone receptor (GHR) gene and protein expression in tendon fibroblasts (PMC6271067) — making local tissue more sensitive to endogenous GH rather than increasing GH output. This is a key distinction: it potentiates existing GH signalling at the repair site without altering systemic hormone levels.
The Speed of Effect
Within 10 minutes of injury, BPC-157 simultaneously increases expression of Akt1, Braf, Egfr, Egr1, Grb2, Mapk1/3/14, Nos3, Ptk2, Pxn, Src, and Vegfa — a broad transcriptional cascade that primes the tissue environment for repair before inflammatory signalling has even fully developed (Frontiers Pharmacol 2021, DOI: 10.3389/fphar.2021.627533).
Nitric Oxide Modulation — Bidirectional
The NO modulation is context-dependent, not directional:
"It modulates nitric oxide bidirectionally — raising blood pressure when too low, lowering it when too high." — BasedBiohacker
This adaptive behaviour distinguishes BPC-157 from conventional vasodilators and is part of why the safety profile across 30 years of animal research has been clean — it doesn't push any single parameter in one direction.
The Gut — Primary Indication and Origin
"The compound that changed it was BPC-157. Chronic gastric ulcers induced with acetic acid. BPC-157 given orally and by injection for 12 days. The treated group's ulcers were nearly fully healed — thick granulation tissue, new glandular epithelium rebuilding from underneath. The peptide outperformed famotidine — the drug in Pepcid — in every model tested. PMID: 15052688"
The gut is where this compound was found, and where the most research exists:
- Gastric and mucosal ulcers — rapid closure, outperforms proton pump inhibitors and H2 blockers in animal models (PMID 15052688)
- Intestinal fistulas — almost nothing closes intestinal fistulas pharmacologically; BPC-157 consistently does in animal studies
- NSAID gut damage — protects the gut lining during NSAID use without blocking their anti-inflammatory effects systemically
- LPS translocation — restores tight junction integrity → reduces endotoxin leakage into systemic circulation
The fistula finding is clinically notable because intestinal fistulas are a significant surgical problem with few non-operative treatment options. BPC-157's effect on fistula closure appears in multiple independent studies, making it one of the more distinctive and harder-to-dismiss results in the literature.
GutOptimized (@GutOptimized) positions BPC-157 in gut repair protocol step 6 — after addressing inflammation, digestion, immune modulation, motility, and oxidative stress. The sequencing matters: BPC-157 is a repair compound, not a first-line anti-inflammatory.
The Gut-Brain Axis — The Underreported Angle
BasedBiohacker (@BasedBiohacker):
"Most see it as gut healing and miss the systemic cognitive enhancement happening when the foundation gets fixed. The gut-brain axis is WAY stronger than people realise."
The neurological effects attributed to BPC-157 in the community — brain fog resolution, mood stabilisation, dopamine receptor restoration — are not primarily direct brain effects. They are downstream consequences of gut repair.
The chain:
flowchart TD
DAMAGE[Damaged gut lining] -->|LPS leaks through| ENDO["Endotoxaemia (systemic LPS)"]
ENDO -->|TLR4 activation| NEURO[Neuroinflammation]
NEURO -->|cytokines reach brain| SYMP["Depression · anxiety · brain fog ·<br/>dopamine downregulation"]
BPC((BPC-157)) -->|restores gut barrier| BLOCK[LPS translocation blocked]
BLOCK -.->|neuroinflammation resolves| NEUROBasedBiohacker on dopamine receptor desensitisation:
"Dopamine receptors downregulate from chronic stimulant use. BPC-157 reverses this receptor desensitisation at the structural level — actually restoring baseline dopaminergic function."
This is the same LPS → insulin resistance → visceral fat pathway described in the lactoferrin deep dive, but here the neurological downstream is the focus rather than the metabolic. Gut barrier integrity is foundational to both.
Beyond the Gut — Documented in Animal Studies
| Tissue | Effect | Notable finding |
|---|---|---|
| Tendon | Outperformed all comparators in tear repair | Organised collagen alignment, full functional restoration |
| Ligament | Accelerated healing (oral dose worked) | Relevant because ligament has poor blood supply normally |
| Bone | Closed defects, matched bone graft performance | Osteogenic via VEGF-driven vascularisation |
| Peripheral nerve | Axonal regrowth through crush injuries | VEGF + growth factor upregulation in nerve sheaths |
| Liver | Reversed alcohol-induced damage | Antioxidant + angiogenic + anti-inflammatory mechanisms |
| Cornea | Sealed puncture wounds | Rapid epithelial and stromal closure |
| Heart | Restored function after induced ischaemia | Angiogenic repair of ischaemic tissue |
| TBI | Structural-level recovery data | One of few compounds with mechanistic TBI data |
The pattern across all these is the same: BPC-157 restores vascular supply → endogenous repair proceeds → tissue-specific cells (tenocytes, hepatocytes, neurons) rebuild under restored conditions.
Oral vs Injectable — The Practical Choice
This is where BPC-157 diverges from most peptides.
Most therapeutic peptides have near-zero oral bioavailability because proteases in the gut degrade them within minutes. BPC-157 is the exception: it was found in gastric juice specifically because it is gastric-stable. It resists degradation at pH 1.2 for 24+ hours. This is intrinsic to its molecular structure.
Oral BPC-157 bioavailability (animal models): ~30–50% — dramatically above typical peptide oral bioavailability of <5%. No published human bioavailability measurement exists.
| Route | Best for | Notes |
|---|---|---|
| Oral (capsule/powder) | Gut healing, systemic effects via gut-brain axis | Direct delivery to gut lining; gastric-stable; onset slower but more sustained |
| Subcutaneous injection | Injury repair (tendon, ligament, muscle, bone), systemic effects | Peak plasma in 15–30 min; higher systemic exposure per dose |
| Intramuscular injection | Site-specific injury | Depot effect in muscle |
For gut conditions specifically, the oral route may be superior to injection — it delivers the peptide directly to the surface that needs repair rather than relying on systemic circulation to redistribute it.
BasedBiohacker's personal protocol: oral, 500mcg (1 capsule) daily for 30-day cycles.
Pharmacokinetics
Published PK data from PMC9794587:
| Route | t½ | Tmax | Bioavailability |
|---|---|---|---|
| IV (rats) | 15.2 min | — | 100% |
| IV (dogs) | 5.27 min | — | 100% |
| IM (rats) | — | 3 min | 14–19% |
| IM (dogs) | — | 6–9 min | 45–51% |
The PK/PD disconnect: plasma half-life is minutes, but pharmacodynamic effects persist days to weeks. Proposed mechanisms: VEGFR2 signalling cascade persistence after the peptide has cleared, local tissue accumulation at injury sites, and transcriptional priming. Once-daily dosing is rational despite the short t½.
Forms: Acetate vs Arginate
| Form | Research support | Notes |
|---|---|---|
| BPC-157 Acetate | All published animal and human studies | The research standard; triple-proline sequence resists pepsin/trypsin |
| BPC-157 Arginate ("stable") | In vitro stability only; patent claims | "90% oral bioavailability" is a patent claim and in vitro result — not a peer-reviewed finding |
The arginate "90% bioavailability" figure appears frequently in commercial marketing. It originates from patent filings and simulated gastric fluid experiments, not from a published human PK study. Until a head-to-head PK comparison appears in a peer-reviewed journal, the acetate form remains the evidence-based choice.
Dosing
No established human dose from clinical trials exists. Community and animal research data:
| Use case | Dose | Route | Notes |
|---|---|---|---|
| Gut healing / systemic | 250–500mcg/day | Oral | BasedBiohacker's protocol: 500mcg × 30 days |
| Acute injury | 250–500mcg/day | Subcutaneous near injury site | Split AM/PM in some protocols |
| Maintenance / prevention | 200–250mcg/day | Oral | Lower end; less data |
| Research protocols | Variable | Both | Zagreb group used 10–100µg/kg in rats |
The 250–500mcg human dose is extrapolated from rat HED calculations. No dose-ranging human trial has established a therapeutic window.
Community Stacks
Classic: BPC-157 + TB-500
The most common pairing in the injury repair community. TB-500 (Thymosin Beta-4) promotes actin polymerisation and cell migration. BPC-157 drives angiogenesis. Together they address the two main rate-limiters of tissue repair: vascularisation and cellular migration into the wound bed.
Typical protocol: 500mcg BPC-157 + 500mcg–2.5mg TB-500, subcutaneous, 2–3× per week for 4–6 weeks.
GutOptimized — Gut Repair Stack
Step 6 of the gut repair protocol: BPC-157, alongside larazotide, GHK, zinc L-carnosine, glutamine, S. boulardii, bone broth. Note the sequencing — BPC-157 enters after inflammation, digestion, and motility are addressed.
BasedBiohacker — Systemic / Cognitive Stack
Oral BPC-157 500mcg/day as the gut-brain axis foundation, layered under cognitive performance compounds. The rationale: cognitive enhancement compounds perform on a healthy substrate — fixing LPS translocation first removes the ceiling on what nootropics can achieve.
Safety and the Cancer Concern
After 30+ years of animal research and no human fatality or LD50 established in any model, BPC-157 has one of the most benign acute safety profiles in the peptide space.
The main concern is theoretical, not observed:
Two mechanistic vectors raise the concern:
Risk vector 1 — VEGF/angiogenesis: BPC-157 upregulates VEGFR2 and drives new blood vessel formation. VEGF/VEGFR2 pathways are active in approximately half of all cancers — tumour angiogenesis is a key hallmark of malignancy. The theoretical risk: BPC-157 could accelerate vascularisation of a pre-existing occult tumour, feeding its growth.
Risk vector 2 — FAK phosphorylation: Elevated FAK activity correlates with lymph node metastasis and poor survival across multiple tumour types (PMID 12838315). BPC-157's FAK-paxillin pathway activation — the same mechanism that drives organised tissue repair — could theoretically accelerate tumour cell migration in someone with active malignancy.
No human case of BPC-157-accelerated cancer has been documented. A 2004 melanoma cell-line experiment showed growth inhibition (single study, unreplicated, in vitro). These two facts sit in tension — the mechanistic concern is real; the observed outcome is not.
The FDA's position (2023): FDA classified BPC-157 as a Category 2 bulk drug substance, citing "insufficient evidence of safety and efficacy" — primarily immunogenicity risk (immune reactions to foreign peptide) and the theoretical VEGF concern. This is a regulatory caution, not a toxicity finding.
Practical risk stratification: - Healthy individuals with no known cancer: theoretical risk only, no observed signal in 30 years - Active or recent cancer: the VEGF concern becomes relevant — angiogenesis promotion is contraindicated in malignancy contexts - Unknown: family history, unscreened individuals — the absence of human safety data means genuine uncertainty
The compound's own research group (Sikiric, Zagreb) published a 2025 response defending BPC-157's safety profile, noting the bidirectional NO modulation is protective against VEGF's cytotoxic actions: PMC12567171
The Research Quality Problem
The most important caveat with BPC-157 is one the community largely ignores: virtually all published research originates from a single group — Professor Predrag Sikiric at the University of Zagreb.
Over 30 years, Sikiric's group has published ~150 papers. Independent replication from unaffiliated laboratories is sparse. The Zagreb group's results are internally consistent and methodologically reasonable, but independent replication is the cornerstone of scientific credibility. No large-scale, double-blind human efficacy RCT exists for any indication.
This does not mean the results are wrong. Animal data is reproducible within the Zagreb group, and the mechanistic pathway (VEGF/NO/angiogenesis) is consistent with established physiology. But it does mean the confidence level is lower than the community enthusiasm often implies.
The limited human data includes: - 2024: n=12 women with interstitial cystitis, 10mg intravesical injections — all patients reported improvement, no short-term adverse effects - 2025: n=2 healthy adults, 10–20mg IV infusion — no organ function marker changes, good tolerability
These are not efficacy trials. They are safety observations in tiny groups.
There is one additional damning data point: NCT02637284 — a Phase I human trial of BPC-157 that completed enrolment in 2015. Eleven years later, results have never been published. The reason for non-publication is unknown; it may reflect negative findings, logistical issues, or commercial suppression. Its absence from the literature is not a finding of harm, but it is a notable gap.
Healthy Alfred (@HealthyAlfred):
"No lethal dose in 30 years. WADA banned it. FDA is now reconsidering it."
WADA's ban reflects performance enhancement potential, not safety concerns — the same logic as colostrum.
What BPC-157 Does Not Do
Community claims outrun the evidence on several fronts:
- "Reverses Parkinson's" — one rat study, Parkinson's model, significant translatability caveats. Not established.
- "Grows hair" — VEGF upregulation in follicles is mechanistically plausible; no controlled hair growth data in humans.
- "Oral is as effective as injectable for injury" — for gut effects, oral is preferred (direct local delivery). For structural injuries (tendon, ligament, bone), injectable delivers higher systemic exposure. The rat ligament study where "oral worked" doesn't establish human equivalence.
- "Raises GH or IGF-1" — BPC-157 upregulates GH receptor sensitivity in fibroblasts, not GH output. It does not increase circulating GH or IGF-1.
- "The arginate form has 90% bioavailability" — this is a patent claim and in vitro finding, not a published human PK study. Treat as unverified marketing.
- "FDA is reconsidering" — FDA's 2023 Category 2 classification is unchanged. No reclassification is underway as of 2026.
- "Builds muscle directly" — not anabolic. No effect on mTOR or androgen receptor. Muscle repair (via restored vascular supply) is different from muscle building.
Legal Status
| Jurisdiction | Status |
|---|---|
| UK | Not a controlled substance (Misuse of Drugs Act 1971). Not scheduled (Psychoactive Substances Act 2016). Legal to possess. Illegal to sell for human consumption without MHRA authorisation. Legal to sell as "research chemical" for laboratory use. |
| US | FDA prohibited from compounding at licensed pharmacies (2023 Category 2 ruling). Not a scheduled substance — possession for personal use is a grey area. Cannot be legally prescribed. |
| EU | Generally unscheduled across member states; regulatory position varies. Not an authorised medicinal product anywhere. |
Sourcing
BPC-157 is a research chemical in most jurisdictions, not approved for human use. It exists in a grey regulatory zone — legal to possess and purchase as a research compound in the UK and most of the EU; legal ambiguity exists around intent.
What to look for: - Certificate of Analysis (CoA) from third-party lab confirming sequence and purity (≥98%) - HPLC purity confirmation — not just mass spectrometry (MS confirms sequence; HPLC confirms actual purity level) - Correct molecular weight on CoA: BPC-157 acetate ~1419 Da - Storage: lyophilised powder, 4°C short-term, −20°C long-term; once reconstituted, use within 2–4 weeks refrigerated
Reconstitution for injection: bacteriostatic water (not sterile water) — allows multi-use. Typical concentration: 500mcg/ml (500mcg vial + 1ml bac water).
Community-cited suppliers: - UK: Peptides Lab UK (peptideslabuk.com), Tide Labs (tidelabs.co.uk), My Peptides (my-peptides.co.uk) - US: Spartan Peptides, Real Peptides, Peptide Sciences (international shipping available)
For UK/EU, community forums (r/Peptides, Longecity) maintain updated sourcing lists as availability changes frequently. Chinese wholesale is the dominant upstream source across most vendors — batch-to-batch contamination and underdosing are documented. HPLC + mass spec certificates are the minimum to verify; endotoxin testing matters for injectables.
Research Sources
Foundation papers: - Original compound description (Sikiric, 1993): PMID 8298609 - Comprehensive review — gut, tendon, CNS, CV (Sikiric, 2018): PMID 29789352 - Brain-gut axis review (Sikiric, 2023): PMID 37242459 - GI comprehensive review (Sikiric, 2024): PMID 38980576
Mechanism: - Early gene expression cascade (Frontiers Pharmacol 2021): DOI 10.3389/fphar.2021.627533 - GH receptor upregulation in tendon fibroblasts: PMC6271067 - Angiogenesis / NO mechanism (2025): PMC12567428 - Angiogenesis / NO safety response: PMC12567171
Tissue healing: - Gastric ulcer healing, outperforms famotidine: PMID 15052688 - Musculoskeletal healing narrative review (2025): PMC12446177 - Ligament healing (oral route): Pentadecapeptide BPC 157 improves ligament healing in the rat — Sikiric group - Bone defect closure: Osteogenic effect of a gastric pentadecapeptide on healing of segmental bone defect in rabbits
Safety / pharmacokinetics: - Pharmacokinetics (rats & dogs): PMC9794587 - FAK and cancer correlation: PMID 12838315 - NCT02637284 — Phase I trial, completed 2015, results unpublished: clinicaltrials.gov
Community resources: - Clinical evidence guide 2026: bodynutrition.org/bpc-157 - 147-study review: klow-peptide.com - Oral vs injectable: spartanpeptides.com - Arginate bioavailability claim analysis: peptidenerds.com - Cancer risk analysis: allaboutpeptides.com
All community quotes compiled from biohacking Twitter discussions. Educational purposes only. Not medical advice. BPC-157 is not approved for human therapeutic use in any jurisdiction.