Dihexa — Deep Dive
Category: Nootropic / Synaptogenic peptide / Neurotrophic mimetic
Full name: N-hexanoic-Tyr-Ile-(6)-aminohexanoic amide (a.k.a. N-(1-oxohexyl)-L-tyrosyl-N-(6-amino-6-oxohexyl)-L-isoleucinamide)
Aliases: PNB-0408; "Dihexa" is a contraction of di-hexa (the two hexanoic appendages)
CAS: 1401708-83-5
Formula / MW: C₂₇H₄₄N₄O₅ · ~504.7 g/mol
Origin: Joe Harding & John Wright's lab, Washington State University — derived from angiotensin IV
Why Dihexa Is the Most Interesting Cautionary Tale in This Database
Most compounds here fall into one of two buckets: "promising but under-evidenced" (BPC-157, Epithalon) or "real drug, mostly-known mechanism" (modafinil, the Russian peptides). Dihexa is something rarer and more instructive — a compound whose headline mechanism, the one repeated in every vendor blurb and every stack thread, rests substantially on a paper that was retracted in 2025 for fabricated data.
That does not make dihexa fake. It makes it the single best worked example in this whole compendium of how to read a hype claim sceptically — because the gulf between what people say about dihexa ("ten million times more potent than BDNF") and what is actually established (a handful of rodent studies, one now retracted, zero human trials) is the widest of any compound we cover.
So this deep dive does two jobs at once. It builds the molecule up honestly from first principles — chemistry, receptor, cell, system — because the story is genuinely elegant. And it runs an unusually hard evidence-calibration pass, because dihexa is where the database's "honest about weak vs strong evidence" promise gets stress-tested.
The bottom line up front: dihexa is a metabolically-stabilised angiotensin-IV fragment that almost certainly does something synaptogenic in rodent hippocampus. Whether it does it through the famous HGF/c-Met mechanism — and whether it is safe in humans, where c-Met is a textbook oncogene — are both genuinely open questions.
Step 1 — The Lineage: From a Blood-Pressure Hormone to a Brain Peptide
To understand the molecule you have to start three steps upstream, with the renin–angiotensin system — the hormonal cascade best known for controlling blood pressure and fluid balance.
The cascade runs: angiotensinogen → angiotensin I → angiotensin II (the famous vasoconstrictor) → and then, by further enzymatic trimming, down to a small C-terminal fragment, angiotensin IV (AngIV), sequence Val-Tyr-Ile-His-Pro-Phe.
For decades AngIV was treated as an inert breakdown product. Then in the 1990s, Harding and Wright's group at WSU showed something unexpected: inject AngIV into rodent brain and you get marked improvements in learning and memory. They proposed a distinct binding site for it — the AT4 receptor — separate from the AT1/AT2 receptors that handle the cardiovascular side of angiotensin signalling.
The AT4 site was later identified as insulin-regulated aminopeptidase (IRAP) — an enzyme, not a classical signalling receptor. This already tells you the mechanism was contested from the very beginning: was AngIV procognitive because it inhibited IRAP (sparing other neuropeptides from degradation), or because it did something else entirely? Hold that thought — the same ambiguity reappears, larger, at the c-Met stage.
flowchart TD
AGT[Angiotensinogen] --> AI[Angiotensin I]
AI --> AII["Angiotensin II<br/>(blood pressure)"]
AII --> AIII[Angiotensin III]
AIII --> AIV["Angiotensin IV<br/>VYIHPF<br/>(procognitive)"]
AIV -->|"binds AT4 site<br/>= IRAP enzyme"| IRAP["IRAP / AT4<br/>(aminopeptidase)"]
AIV -->|"WSU re-engineering"| DIH["Dihexa<br/>(metabolically stable,<br/>oral, brain-penetrant)"]
IRAP -.->|"mechanism contested<br/>from the start"| DIHThe lineage: dihexa is the great-grandchild of the blood-pressure hormone angiotensin II, engineered out of the procognitive fragment AngIV.
The engineering problem AngIV had
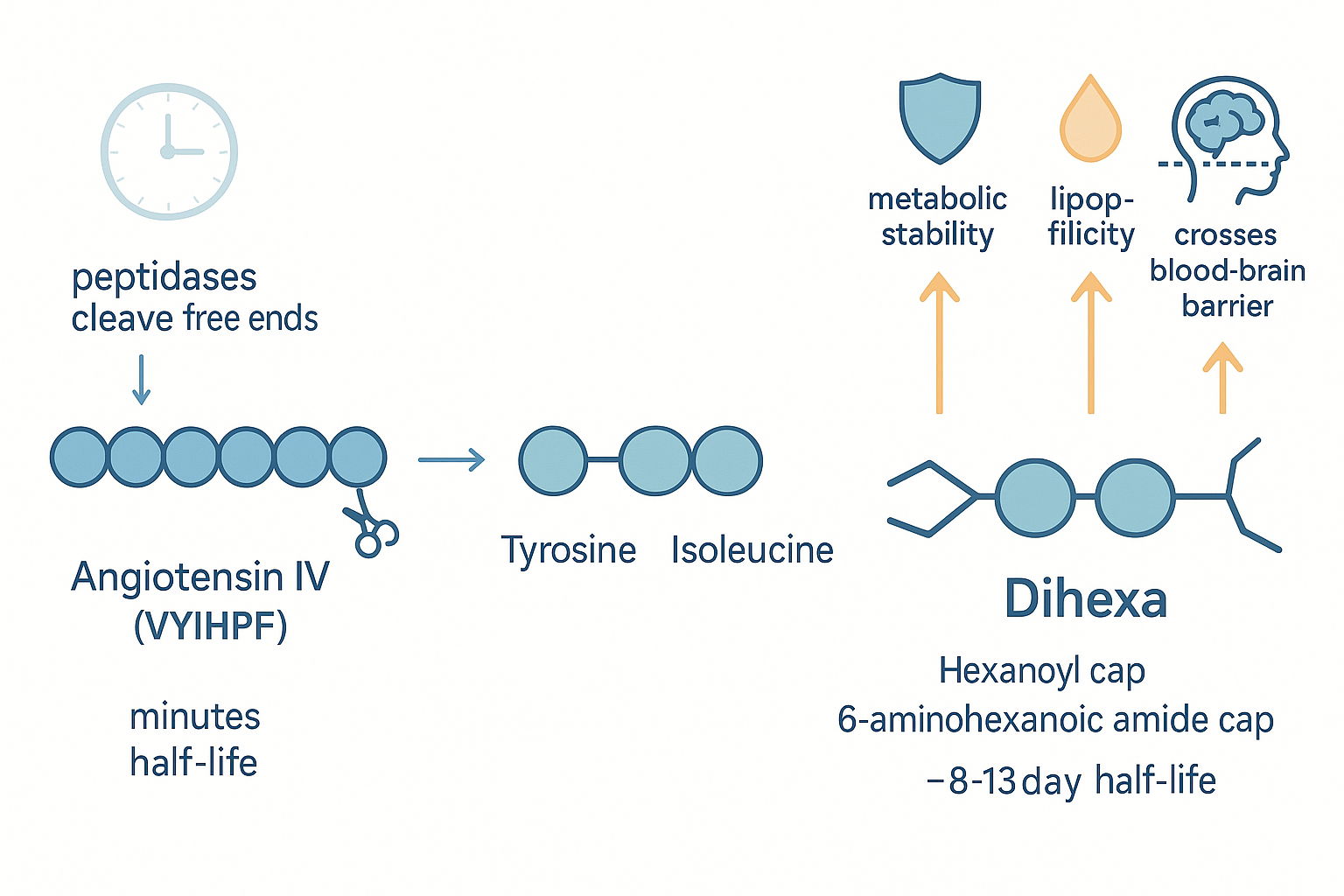
AngIV works in the brain but is useless as a drug: it is a small peptide, so peptidases shred it within minutes, and it does not cross the blood–brain barrier when given systemically. To get an effect you had to inject it directly into the brain (intracerebroventricular). That is fine for a mechanism paper, hopeless for a therapeutic.
Dihexa is the solution to exactly that problem. The WSU group stripped AngIV down to its two pharmacophore residues — tyrosine and isoleucine — and then capped each end with a six-carbon (hexanoic / hexyl) chain:
- an N-terminal hexanoyl group (a six-carbon acyl cap), and
- a C-terminal 6-aminohexanoic amide tail.
Those two hexa-appendages are where the name comes from, and they do three things at once.
Step 2 — The Molecule: Why Two Fatty Tails Change Everything
 From a fragile six-residue peptide to a drug-like molecule: the two hexanoic caps are the entire trick.
From a fragile six-residue peptide to a drug-like molecule: the two hexanoic caps are the entire trick.
The two fatty caps are not decoration — they are the reason dihexa is orally active where AngIV is not:
1. Metabolic stability. Peptidases recognise free N- and C-termini. By blocking both ends with non-peptide caps, dihexa becomes resistant to the aminopeptidases and carboxypeptidases that destroy native AngIV. The payoff is dramatic: in rats, dihexa's plasma half-life is reported on the order of ~8–13 days (McCoy et al. 2013, PMID 23055539) — versus minutes for AngIV. (Treat the multi-day figure with some caution — it comes from the same lab whose work later drew integrity concerns — but the qualitative point, that the caps massively extend stability, is sound chemistry.)
2. Lipophilicity → brain penetration. Those hexyl chains make the molecule strongly fat-soluble. The octanol/water partition coefficient is roughly ~178 — i.e. it strongly prefers lipid over water. A lipophilic small molecule can slip across the blood–brain barrier and through gut epithelium passively. This is why dihexa, unlike its parent, is reported to be orally active and BBB-permeant — the property that made it interesting as a drug at all.
3. The flip side — it barely dissolves in water. The same lipophilicity that gets it into the brain makes it a nightmare to formulate. Aqueous solubility is poor; it dissolves well only in DMSO (~20 mg/mL) and badly in everything biocompatible. This single physico-chemical fact drives almost every practical decision downstream — why community users dissolve it in DMSO and rub it on (transdermal), why dosing is finicky, and why "did the dose even get in?" is a live question for every anecdote.
So at the molecular level dihexa is coherent and clever: take the active core of a procognitive peptide, armour both ends, make it greasy enough to reach the brain. Nothing controversial yet. The controversy is entirely about what it does once it gets there.
Step 3 — The Receptor Story: HGF / c-Met (and Why It's Shaky)
Here is the mechanism you will read everywhere, stated as fact:
Dihexa binds hepatocyte growth factor (HGF) with high affinity, promotes HGF's dimerisation, and thereby potentiates signalling through HGF's receptor, c-Met — driving synaptogenesis.
HGF/c-Met is a real and important system. HGF is a growth factor; c-Met is its receptor tyrosine kinase. In the brain, HGF/c-Met signalling genuinely does support neuronal survival, dendritic growth and synapse formation. So the story is biologically plausible: dihexa as an HGF "potentiator" that turns up an endogenous pro-synaptic growth-factor system.
The cascade, as proposed:
flowchart TD
DIH((Dihexa)) -->|"binds HGF<br/>Kd ~65 pM*"| HGF[HGF dimerises]
HGF -->|"activates"| MET["c-Met receptor<br/>tyrosine kinase"]
MET --> PI3K["PI3K → Akt"]
MET --> MAPK["Ras → MAPK/ERK"]
PI3K --> SPINE["Dendritic spine formation<br/>(spinogenesis)"]
MAPK --> SPINE
SPINE --> SYN["New functional synapses<br/>(synaptogenesis)"]
SYN --> LTP["Hippocampal LTP<br/>↑ learning & memory"]
MET -.->|"oncogene pathway —<br/>see Safety"| CANCER[["c-Met drives tumour<br/>growth & metastasis"]]*The Kd = 65 pM figure and the HGF-dependence experiments come from Benoist et al. 2014 — the paper retracted in 2025 for fabricated data. Read the whole cascade through that lens.
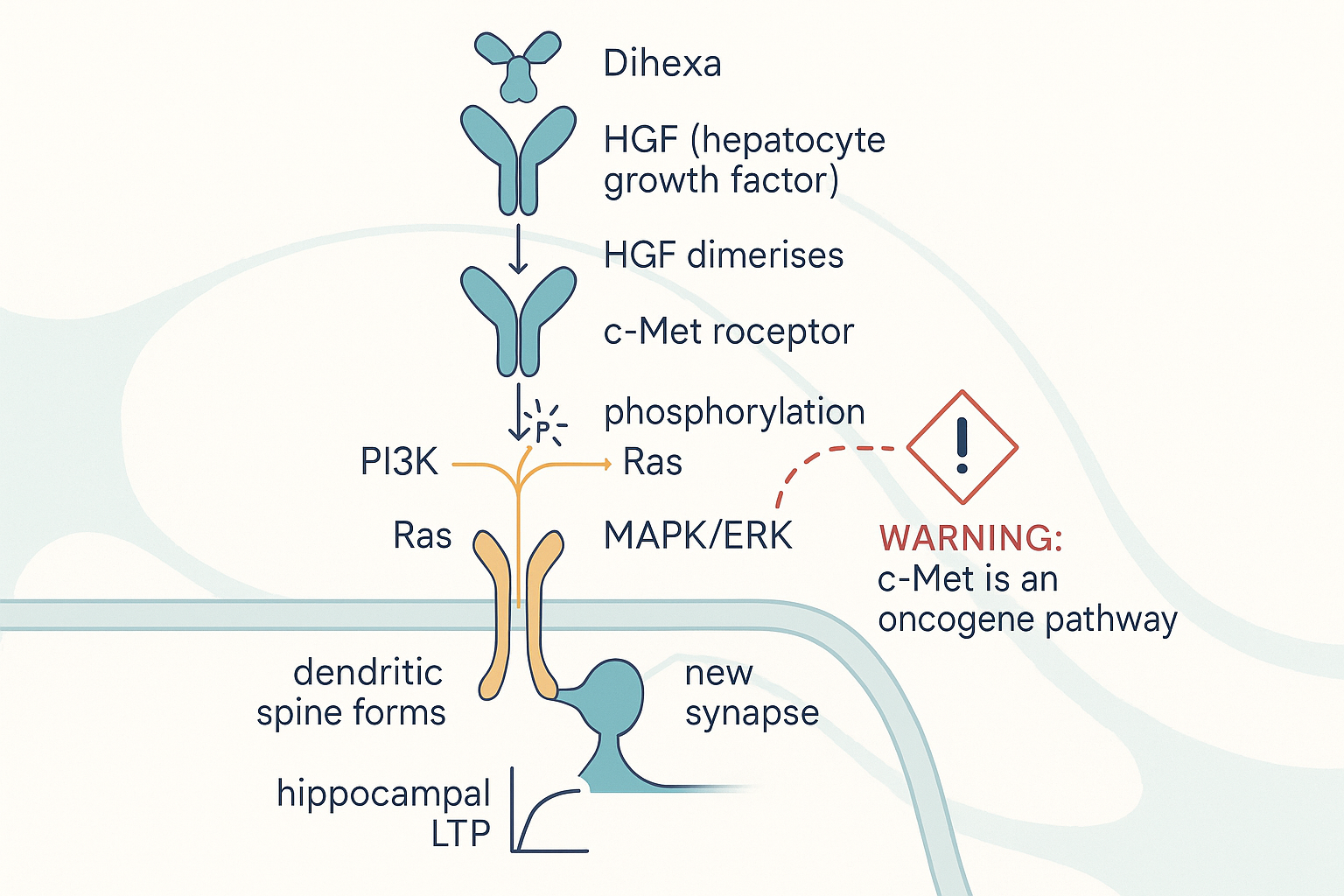 The proposed HGF/c-Met synaptogenesis cascade — and the red side-branch that makes it worrying: the very pathway dihexa is meant to potentiate is a textbook oncogene route.
The proposed HGF/c-Met synaptogenesis cascade — and the red side-branch that makes it worrying: the very pathway dihexa is meant to potentiate is a textbook oncogene route.
Where this came from — and why it broke
The HGF/c-Met mechanism rests primarily on two Harding-lab papers:
- McCoy et al. 2013 (PMID 23055539) — the foundational characterisation: dihexa is orally active, BBB-permeant, and rescues memory in aged and scopolamine-impaired rats. Not retracted. An expression of concern has circulated, but as of 2026 the paper stands.
- Benoist et al. 2014 (PMID 25187433) — "The procognitive and synaptogenic effects of angiotensin IV–derived peptides are dependent on activation of the HGF/c-Met system." This is the paper that nailed the mechanism: it reported dihexa binding HGF saturably with Kd ≈ 65 pM, that synaptogenesis occurred at picomolar (10⁻¹² M) concentrations, and — crucially — that the effect was abolished when you blocked HGF (with an HGF antagonist) or knocked down c-Met (shRNA). That dependence experiment is the entire basis of the "it works through HGF/c-Met" claim.
Benoist 2014 was retracted in April 2025. Washington State University's integrity investigation concluded that figures in this and several related papers contained "falsified and/or fabricated" data, attributing responsibility to Leen Kawas (a Harding PhD student) and Joseph Harding. Kawas had her PhD revoked; she had earlier resigned (2021) as CEO of Athira Pharma — the company spun out to commercialise the chemistry — and Athira settled securities-fraud claims for ~$10M in 2023. An earlier 2012 paper framing these molecules as HGF-dimerisation mimetics was also retracted.
⚖️ Calibration — the mechanism you read everywhere is the part that was fabricated
The picomolar Kd, the saturable HGF binding, and the c-Met-dependence experiments — i.e. the specific evidence that dihexa works via HGF/c-Met — are exactly the data that did not survive scrutiny. What plausibly survives the retraction is weaker and more generic: that dihexa is a metabolically stable AngIV analogue that improves memory in some rodent models. The leap from "improves rodent memory" to "high-affinity HGF potentiator" is the leap that broke.
Is there any surviving mechanistic evidence?
A little, and it points elsewhere. An independent Chinese group (Sun et al. 2021, PMID 34827486) reported that dihexa rescued cognition in APP/PS1 Alzheimer's-model mice — but attributed it to PI3K/Akt signalling, without re-establishing the HGF-binding step. So the most robust independent replication of a dihexa effect does not confirm the famous mechanism. The honest summary: an effect signal exists in rodents from more than one lab; the HGF/c-Met causal chain specifically is, at best, unconfirmed and, at worst, built on retracted data.
Step 4 — The Cell: Synaptogenesis and Dendritic Spines (the genuinely interesting bit)
Set the mechanism controversy aside for a moment and look at what dihexa is claimed to do at the cellular level, because this is what makes it conceptually distinct from every other "neurotrophic" compound in this database.
Most cognitive compounds modulate neurotransmission — they change how existing synapses fire (cholinergic, dopaminergic, glutamatergic tone). A smaller set are neurotrophic — they raise growth factors (Semax raising BDNF; cerebrolysin's neurotrophic peptide fraction). Dihexa's claim is more aggressive still: it is a synaptogenic agent — it is supposed to drive the physical construction of new synapses.
The relevant cellular currency is the dendritic spine — the tiny membranous protrusion on a dendrite that houses an excitatory synapse. More spines ≈ more synaptic connections ≈ greater capacity to encode information. In the (retracted) culture work, subthreshold HGF plus picomolar dihexa drove spine counts up synergistically — from ~18 to ~27 spines per 50 µm of dendrite — and these new spines were functional (they supported synaptic transmission). At the systems level this maps onto long-term potentiation (LTP) in the hippocampus — the cellular substrate of learning.
This is why the community frames dihexa as forced neuroplasticity rather than mere stimulation:
flowchart LR
subgraph Neurotransmission["Modulate firing"]
A["modafinil, racetams,<br/>guanfacine"]
end
subgraph Neurotrophic["Raise growth factors"]
B["Semax (BDNF),<br/>cerebrolysin"]
end
subgraph Synaptogenic["Build new synapses"]
C["Dihexa<br/>(claimed)"]
end
A --> EFFECT["Cognitive effect"]
B --> EFFECT
C --> EFFECT
C -.->|"rapid, structural,<br/>indiscriminate?"| RISK["Top-down control<br/>concern"]Three altitudes of "cognitive enhancement." Dihexa claims the highest-leverage and least-reversible one — physically rewiring connectivity — which is also why a careful biohacker is most wary of it.
The "structural, not just functional" claim is exactly what makes dihexa attractive (durable rewiring rather than a transient boost) and exactly what makes the more thoughtful users nervous (see aestheticprimal's caution below). Building synapses indiscriminately is not obviously a good thing if you cannot control which synapses.
Step 5 — The Systems Level: Memory, and the Clinical Reality Check
In rodents, the systems-level signal is consistent across the (admittedly thin and partly-compromised) literature: aged or pharmacologically-impaired rats given oral dihexa perform like healthy controls on the Morris water maze (the standard rodent spatial-memory test). McCoy 2013 reported this at ~2 mg/kg/day orally. There are also scattered reports in Huntington's-like and Parkinson's-like rodent models.
Then the literature simply stops at the species boundary.
⚖️ Calibration — the human evidence base is empty
There are zero published placebo-controlled human trials of dihexa. Not "small," not "preliminary" — zero. Every human report is an anecdote from a research-chemical user. Everything below the rodent line is extrapolation.
The closest thing to a clinical readout comes from the drug-development sibling, not dihexa itself. The chemistry was advanced commercially via M3 Biotechnology → Athira Pharma, whose lead clinical candidate fosgonimeton (ATH-1017) — a phosphate pro-drug in the same HGF/c-Met "positive modulator" program — went into Alzheimer's trials. In September 2024, Athira's Phase 2/3 LIFT-AD trial missed its primary endpoint. Athira subsequently laid off most of its staff and exited neuroscience. That is the only time this mechanistic family has been tested at clinical scale in humans, and it failed.
So the honest systems-level statement is: dihexa improves memory in rodents; the broader HGF/c-Met cognitive thesis failed its one real human test; and dihexa itself has never been tested in a human trial at all.
flowchart TD
CLAIM["CLAIM:<br/>'10 million times more<br/>potent than BDNF'"] --> SRC["SOURCE:<br/>in-vitro spine assay,<br/>Harding-lab papers"]
SRC --> RETRACT["Mechanism paper<br/>RETRACTED 2025<br/>(fabricated data)"]
EVID["WHAT'S ACTUALLY SHOWN:"] --> R1["Rodent memory rescue<br/>(McCoy 2013, not retracted)"]
EVID --> R2["Rodent rescue via PI3K/Akt<br/>(Sun 2021, independent)"]
EVID --> R3["Sibling drug fosgonimeton<br/>FAILED Phase 2/3 (2024)"]
EVID --> R4["Human dihexa trials: ZERO"]
EVID --> R5["Carcinogenicity studies: ZERO"]The "claim vs evidence" map. The arresting potency number traces to assays in retracted papers; the durable evidence is rodent-only and the one human-scale test of the mechanism failed.
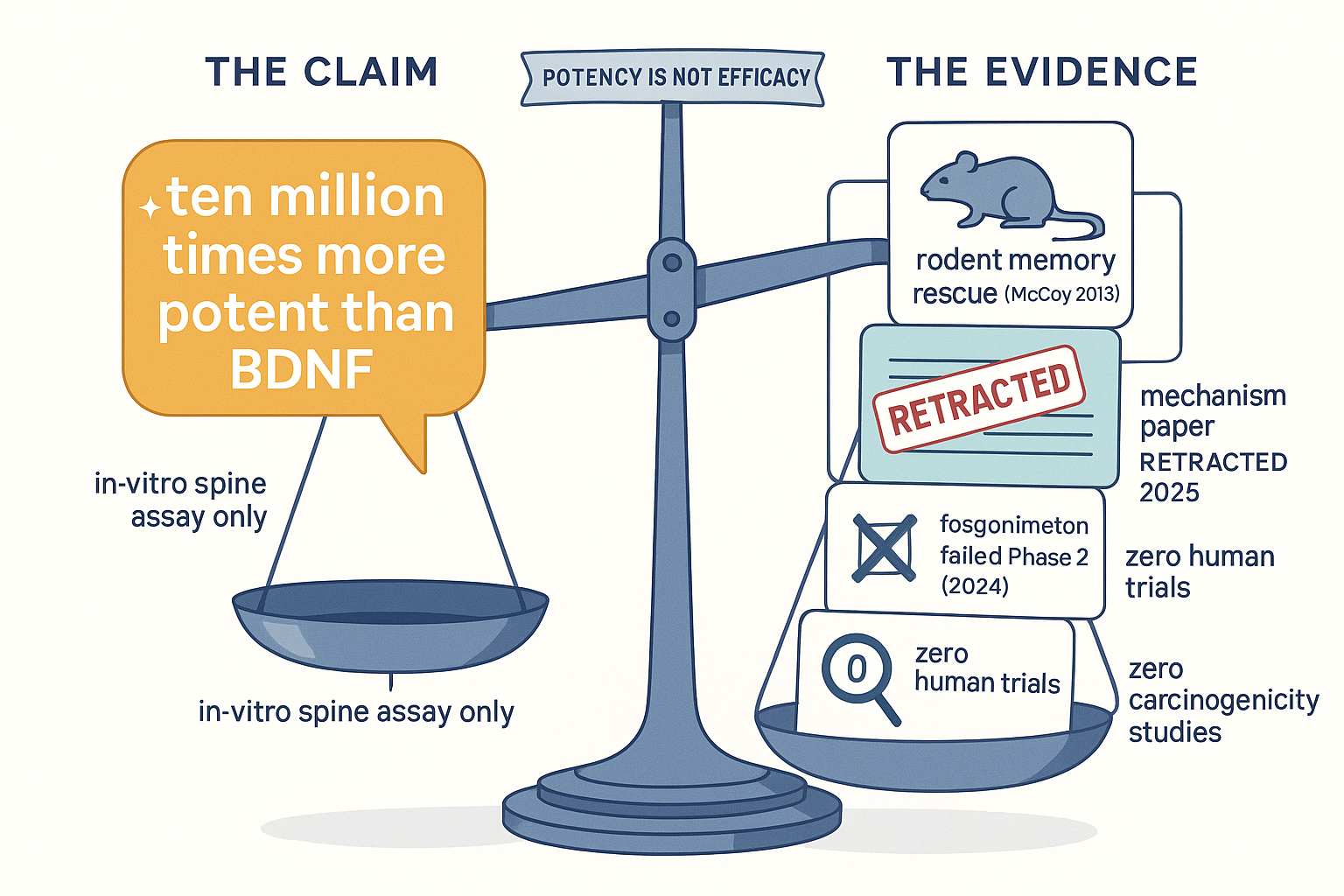 The hype on one pan, the evidence on the other: a single in-vitro potency number versus rodent-only data, a retracted mechanism paper, a failed human trial, and no cancer studies.
The hype on one pan, the evidence on the other: a single in-vitro potency number versus rodent-only data, a retracted mechanism paper, a failed human trial, and no cancer studies.
How to read "ten million times more potent than BDNF"
This is the line that sells dihexa. Unpack it carefully:
- It is a comparison of molar potency at one narrow in-vitro endpoint (concentration needed to drive spine formation in cultured neurons): dihexa active at picomolar, BDNF at nanomolar → ~7 orders of magnitude ≈ "ten million times."
- Potency is not efficacy, and it is not relevance. Needing fewer molecules to trip one assay says nothing about whether the downstream cognitive effect is larger, or even present, in a human brain. BDNF is a pleiotropic master-regulator acting through TrkB across countless circuits; dihexa tripping one spine-count assay at low concentration is not "ten million times better at making you smarter." It is a category error dressed as a spec sheet.
- And the assays generating the number sit in the papers now under retraction / concern.
Treat "ten million times more potent than BDNF" the way you'd treat "0–60 in 2 seconds" printed on a car that has never been driven outside the factory.
Step 6 — Safety: The c-Met Oncogene Problem Is Not Hypothetical Hand-Waving
Every compound in this database gets a cancer-caveat paragraph. Dihexa's is the one to take most seriously, for a precise reason: c-Met is one of the most thoroughly characterised oncogenes in human biology.
The HGF/c-Met axis — the exact pathway dihexa is claimed to potentiate — drives tumour proliferation, invasion, angiogenesis and metastasis across lung, liver, gastric, breast, kidney and other cancers. This is so well established that the FDA has approved c-Met inhibitors (capmatinib, 2020; tepotinib, 2021) as anticancer drugs. In other words: an entire class of oncology medicines exists to do the opposite of dihexa's proposed action.
This produces an uncomfortable logical fork:
- If the HGF/c-Met mechanism is real, then dihexa is a systemically-distributed, long-half-life, brain-penetrant c-Met potentiator — and chronically nudging a master oncogene pathway upward, especially in anyone with an undetected pre-malignant clone, is exactly the kind of thing oncologists spend their careers trying to prevent.
- If the HGF/c-Met mechanism is not real (because the supporting data were fabricated), then dihexa's true mechanism is unknown — and you are dosing an uncharacterised research chemical with no idea what it actually does.
Neither branch is reassuring. And the empirical backstop is missing: no carcinogenicity studies have been conducted on dihexa. The "no apparent toxicity in short-duration studies" line that appears in vendor copy refers to brief rodent dosing — it tells you nothing about multi-year cancer risk in humans, which is precisely where a c-Met agonist would show its hand.
Add the mundane unknowns: no human pharmacokinetics, a multi-day half-life meaning the drug accumulates with daily dosing, no established therapeutic window, and a compound so lipophilic that dose delivery is itself uncertain.
⚖️ Calibration — the honest safety verdict
Dihexa has no documented human toxicity because almost no humans have been studied, not because it has been shown safe. The single most-cited mechanism is also a textbook cancer pathway, carcinogenicity has never been tested, and the half-life invites accumulation. This is the compound in this database where "absence of evidence is not evidence of absence" matters most.
Step 7 — Practical Reality: Sourcing, Routes, Dosing
Dihexa is a research chemical — not an approved drug anywhere, sold "for laboratory research only." Everything here is descriptive, not a recommendation.
Routes — driven entirely by the solubility problem
Because dihexa is barely water-soluble, formulation dominates practice:
| Route | How | Notes |
|---|---|---|
| Oral | Powder in capsule, or in lipid/DMSO vehicle | McCoy 2013 established oral activity in rats — the strongest precedent. Lipophilic enough to absorb. |
| Transdermal (DMSO) | Dissolved in DMSO, applied to skin | Most common community route. DMSO solubilises it and carries it through skin. Crude, irritating, dosing imprecise. |
| Intranasal | In DMSO/solvent, sprayed | Used by some (Morph reports "5 mg IN dihexa"). Attempts nose-to-brain delivery (see Semax/Selank for that route's logic). |
| Subcutaneous | Reconstituted in DMSO/bacteriostatic water | Less common; the DMSO requirement makes injection unappealing. |
Dosing anecdotes (no clinical basis whatsoever)
Community doses cluster around 5–10 mg/day, occasionally lower. Note the disagreement that runs through our own ingested sources: some explicitly prefer a low dose.
- Morph runs 5 mg in his "autistic cognition" stack (source) and 5 mg intranasal in his research-flow stack — but elsewhere lists "Dihexa (low dose — recovery)" (source), suggesting the low-dose, neuroprotective framing rather than maximal synaptogenesis.
- Because of the multi-day half-life, frequency matters more than dose: daily dosing accumulates. Many users run short cycles (e.g. a couple of weeks) precisely to avoid open-ended accumulation of an uncharacterised, oncogene-adjacent molecule. The cautious read of the half-life is "dose intermittently, don't stay on it."
Quality markers
If sourcing as a research chemical: third-party Certificate of Analysis, HPLC purity (≥98%) and mass-spec confirmation of the correct mass (~504.7), and an honest vendor about the DMSO-only solubility. The lipophilicity makes underdosed or impure product hard to detect by eye — the powder dissolving cleanly in water is a red flag, not a green one.
How This Fits the Rest of the Database
Dihexa occupies a specific and contrarian niche in our compound landscape: the "rapid, forced, structural neuroplasticity" corner. That framing is what the X/biohacker community gets right and what its more careful members are wary of.
The clearest community endorsement is BasedBiohacker's viral "rabbit hole" tweet, which slots dihexa in as the brute-force answer to a cognitive complaint:
"...can't focus and no supplement is helping? modafinil. you're stupid and no supplement is helping? dihexa. can't sleep and no supplement is helping? silexan... the answer is always just deeper down the rabbit hole."
That is dihexa's reputation in one line: the compound you reach for when ordinary nootropics have failed — the deepest point of the rabbit hole. The same thread's replies route other complaints to other tools — "brain fog? → bpc-157 fix your gut" and "procrastination? → cerebrolysin" — which usefully positions dihexa against its neighbours: it is the structural-rewiring option, distinct from BPC-157's gut-axis repair and cerebrolysin's broad neurotrophic-peptide support.
But the most valuable community signal is the dissent. aestheticprimal — one of the more mechanistically literate voices we ingest — flags exactly the right concern:
"not a fan of things that rapidly induce neuroplasticity because they very often mess up top-down control from the prefrontal cortex, it's why i am a bit cautious of Dihexa, low dose probably different tho. Cortexin is nice, but I'd say Pinealon is even more potent for cognition."
This is a genuinely sophisticated point and worth dwelling on. Indiscriminate, rapid synapse-building is not self-evidently good: the prefrontal cortex exerts top-down control by maintaining a particular, learned pattern of connectivity. A compound that forces new spines everywhere at once could degrade that hard-won structure — strengthening noise along with signal. It is the same intuition that makes thoughtful people cautious about high-dose psychedelics' "everything is connected to everything" plasticity. aestheticprimal's preference for Pinealon and Cortexin over dihexa is the graded-vs-forced distinction in action.
That contrast is the spine of how dihexa relates to its neighbours:
| Compound | Neuroplasticity style | Mechanism altitude | Reversibility |
|---|---|---|---|
| Dihexa | Rapid, forced, structural | Builds synapses (claimed HGF/c-Met) | Low — physical rewiring |
| Semax | Graded, endogenous | Raises BDNF/TrkB | Moderate |
| Pinealon / Epithalon | Slow, regulatory | Epigenetic / neuroprotective | High |
| Cerebrolysin | Broad, trophic | Neurotrophic peptide mixture | Moderate |
| BPC-157 | Indirect (gut-brain) | Angiogenesis / barrier repair | High |
The pattern: dihexa sits at the most aggressive, least reversible, least-evidenced corner of the neuroplasticity space. Semax nudges the brain's own BDNF; the Khavinson peptides regulate gently; dihexa is claimed to pick up the bricks and build. That is precisely why it is the one that demands the most caution.
The community pairings reinforce the "construction" framing rather than the "stimulation" one. aestheticprimal: "dihexa + nicotine = elite writing & memory" — nicotine providing the acute cholinergic firing while dihexa (notionally) lays down structure. Morph repeatedly stacks it with intranasal insulin (memory consolidation) and guanfacine (which reduces prefrontal noise — arguably a deliberate counter-weight to exactly the "top-down control" concern aestheticprimal raised). And it recurs in BasedBiohacker's "stuff I have coming in" haul (source) — i.e. it is widely acquired and experimented with, which is a very different thing from validated.
That is the database's honest position on dihexa in one sentence: the community treats it as the heavy artillery of neuroplasticity; the evidence treats it as an interesting rodent compound with a retracted mechanism and an unstudied cancer flank.
Bottom Line
- What's real: dihexa is a genuinely clever piece of medicinal chemistry — angiotensin IV's active core, double-capped with hexanoic chains to make it stable, lipophilic, oral and brain-penetrant. In rodents it improves memory, and that signal appears from more than one lab.
- What's broken: the famous mechanism — high-affinity HGF binding, picomolar c-Met potentiation, "ten million times more potent than BDNF" — rests on Harding-lab papers, the central one of which (Benoist 2014) was retracted in 2025 for fabricated data. The one human-scale test of this mechanistic family (Athira's fosgonimeton) failed Phase 2/3 in 2024.
- What's unknown and serious: zero human trials of dihexa, zero carcinogenicity studies, a multi-day accumulating half-life, and a proposed mechanism that is a textbook oncogene pathway with FDA-approved inhibitors used to treat cancer.
- The calibrated verdict: dihexa is the clearest worked example in this database of why a striking potency number and a clean mechanistic story should raise your scepticism, not lower it. If you use it, the rational posture is low-dose, short-cycle, and clear-eyed that you are an n-of-1 experiment on an uncharacterised compound whose headline mechanism doubles as a cancer pathway. This is not a "probably fine, under-hyped gem" like some peptides here. It is genuinely high-uncertainty in both directions.
Research Sources
Primary (rodent) literature: - McCoy et al. 2013 — metabolically-stabilised AngIV analogues; oral, BBB-permeant, memory rescue in aged rats. Foundational, not retracted: PMID 23055539 - Benoist et al. 2014 — HGF/c-Met dependence; Kd ≈ 65 pM; picomolar synaptogenesis. RETRACTED April 2025: PMID 25187433 / PMC4201273 - Sun et al. 2021 — independent cognitive rescue in APP/PS1 mice via PI3K/Akt (mechanism not HGF-confirmed): PMID 34827486
Mechanism, controversy & clinical: - Athira / fosgonimeton (ATH-1017) LIFT-AD Phase 2/3 failure, Sept 2024 — the only human-scale test of the HGF/c-Met cognition thesis - WSU research-integrity findings; Kawas/Harding retractions; Athira securities settlement (2023) - c-Met as oncogene; FDA-approved c-Met inhibitors capmatinib (2020), tepotinib (2021)
Background & balanced assessment: - Wikipedia: Dihexa (chemistry, lineage, developer history) - Alzheimer's Drug Discovery Foundation — Cognitive Vitality: Dihexa report (PDF) - Retraction/status overview: peptideprotocolwiki.com
All community quotes compiled from biohacking Twitter/X discussions. Educational purposes only. Not medical advice. Dihexa is an unapproved research chemical with no human safety or efficacy data; its most-cited mechanism rests partly on retracted research, and it acts on a pathway with established oncogenic potential.