The Liver: The Body's Central Processing Unit
Why almost everything you absorb passes through the liver first, and what it does there — buffering your blood sugar, building and breaking your fats and proteins, activating your thyroid hormone, making your bile, and neutralising drugs, toxins and alcohol.
Why this page exists
The two previous foundations pages keep arriving at the same door. The digestion page showed that almost everything water-soluble you absorb — sugars, amino acids, fructose, alcohol, most drugs — is routed onto the portal vein, which goes to the liver before the rest of the body. The cellular energy page showed that glucose and fat are the fuels every cell runs on. The liver is the organ standing between those two facts: it is the central depot that receives the raw absorbed material, decides what to store, what to release, what to transform, and what to destroy, and then dispatches the results to the rest of you.
It is, by a wide margin, the most metabolically versatile organ in the body — performing several hundred distinct chemical jobs. This page does not list all of them. It covers the handful that explain the most: blood-sugar buffering, fat handling, protein handling, bile, detoxification, thyroid activation, and alcohol. Understanding these makes a huge amount of biohacking discourse — fatty liver, "liver support," thyroid conversion, fructose, detox — suddenly legible.
We start, as always, with the plumbing.
The architecture: a chemical plant with two inflow pipes
Most organs receive blood from one artery. The liver is unusual: it has two blood supplies, and the reason matters.
- The hepatic portal vein (~75% of incoming blood). This is the vein we met in the digestion page — it carries nutrient-rich, oxygen-poor blood straight from the gut. Everything just absorbed from your last meal arrives here first. This is the liver's raw material pipe.
- The hepatic artery (~25%). This carries normal oxygen-rich blood from the heart, supplying the liver cells with the oxygen they need to do their energy-hungry work. This is the liver's power pipe.
These two streams mix together and trickle past the working liver cells (called hepatocytes) through tiny leaky channels called sinusoids. The leakiness is deliberate: it lets the hepatocytes sample, extract, and modify whatever is flowing past — pulling glucose out of the blood, dumping newly-made proteins in, grabbing a toxin for disposal. After processing, the cleaned blood collects into the hepatic vein, which carries it out to the general circulation.
There is one more output pipe, and it goes the other way: the bile duct. While blood flows in through the portal vein and out through the hepatic vein, the hepatocytes also secrete bile in the opposite direction, into tiny canals that drain toward the gut. So the liver has three connections to the rest of the body: two pipes in (portal vein, hepatic artery), one pipe out to the blood (hepatic vein), and one pipe out to the gut (bile duct).
flowchart LR
GUT[Gut] -->|"portal vein<br/>(nutrients, ~75%)"| LIVER
HEART[Heart] -->|"hepatic artery<br/>(oxygen, ~25%)"| LIVER
subgraph LIVER["LIVER (hepatocytes + sinusoids)"]
H[Process: store / release /<br/>transform / destroy]
end
LIVER -->|hepatic vein| CIRC[General circulation → body]
LIVER -->|bile duct| BILE[Bile → gallbladder → gut]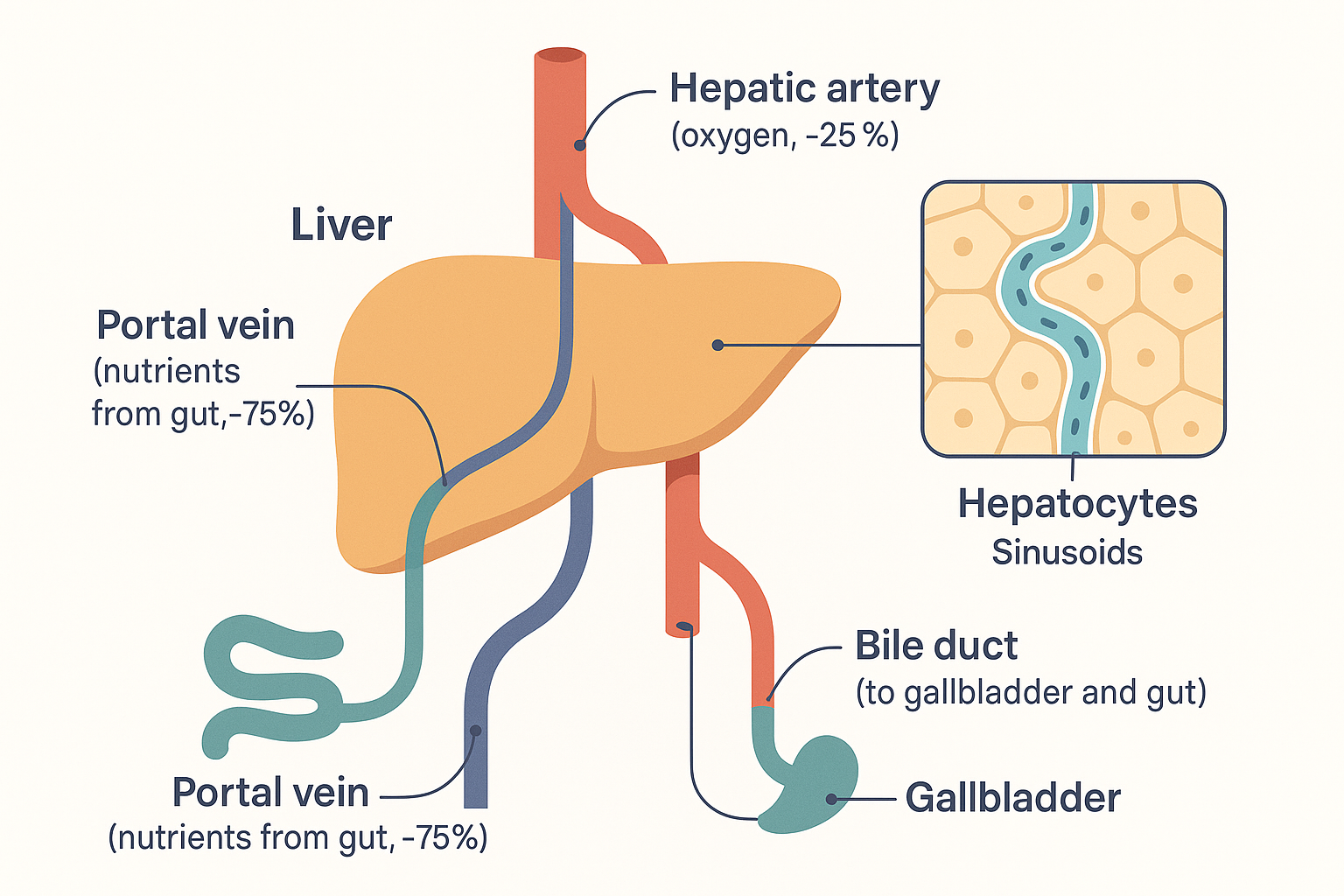 Two pipes in (nutrient-rich portal vein, oxygen-rich hepatic artery), one blood pipe out (hepatic vein), one bile pipe out to the gut — the plumbing that puts the liver first in line.
Two pipes in (nutrient-rich portal vein, oxygen-rich hepatic artery), one blood pipe out (hepatic vein), one bile pipe out to the gut — the plumbing that puts the liver first in line.
This "everything comes here first" position is what makes the liver the body's central processing unit. Now let us walk through what it actually does with the material.
Job 1: Buffering blood sugar — the glycogen battery
Your blood glucose must stay within a narrow band: too low starves the brain (which runs almost entirely on glucose), too high damages tissues. The liver is the principal buffer that keeps it steady between meals — it soaks up glucose when there is a surplus and releases it when there is a shortfall.
It does this with a storage molecule called glycogen — a large branching chain of glucose units, essentially the animal equivalent of starch. Think of it as a rechargeable glucose battery.
- After a meal (glucose high, insulin high): the hormone insulin signals "fuel is plentiful, store it." The liver pulls glucose out of the incoming portal blood and links the units together into glycogen. This process is called glycogenesis (glycogen-making). The liver can hold roughly 100 grams of glucose this way — enough to cover the body's needs for a number of hours.
- Between meals or during fasting (glucose falling, insulin low): the hormones glucagon (the mirror-image of insulin, also from the pancreas) and adrenaline signal "release fuel." The liver breaks glycogen back down into glucose and exports it into the blood. This reverse process is called glycogenolysis (glycogen-splitting).
Notice the symmetry, and notice who controls it: insulin stores, glucagon and adrenaline release. This is the body's short-term blood-sugar thermostat. (Muscle also stores glycogen — about 400g — but muscle is selfish: it keeps its glycogen for its own use and cannot release glucose back into the blood. Only the liver acts as a blood-sugar bank for the whole body.)
How does the glucose physically cross into and out of the liver cell? Through a door called GLUT2 — the liver's glucose transporter. Unlike the insulin-gated GLUT4 doors on muscle and fat (see cellular energy), GLUT2 is always open, low-affinity, and bidirectional: it only moves glucose in bulk when blood glucose is high, and it lets glucose pass in either direction. That single property is what makes the liver a buffer rather than a hoarder — glucose flows in through GLUT2 when blood sugar is high (to be stored as glycogen), and flows back out through the same door when the liver breaks glycogen down or manufactures new glucose. The hormones decide whether to store or release; GLUT2 is simply the ungated turnstile the glucose passes through. (The same low-affinity GLUT2 sits on the pancreas's insulin-releasing cells, which is how the pancreas "reads" blood sugar in the first place — it is the body's glucose sensor as well as the liver's door.)
Job 2: Making glucose from scratch — gluconeogenesis
The glycogen battery only lasts so long. During a longer fast, overnight, or sustained stress or low-carb eating, the ~100g runs down. To keep the brain supplied, the liver switches on a second capability: it manufactures brand-new glucose from non-sugar raw materials. This is gluconeogenesis (literally new-glucose-making).
The raw materials it builds glucose from include:
- Lactate — the molecule muscles produce during hard anaerobic effort (from the cellular energy page); the liver recycles it back into glucose.
- Glycerol — the backbone left over when stored fat (triglycerides) is broken apart.
- Amino acids — particularly alanine, scavenged from muscle protein breakdown when fasting is prolonged (which is part of why extended fasting eventually costs muscle).
This is a defining liver function: it means your blood sugar can be maintained even with zero carbohydrate intake, because the liver will simply build the glucose your brain needs. It is also why "low blood sugar" is rarely a simple fuel-shortage problem and more often a signalling problem — the liver can almost always make more if the hormonal signals are right.
flowchart TD
FED["FED state<br/>(insulin high)"] -->|glycogenesis| STORE[Store glucose as glycogen]
FED -->|"fat & sugar surplus"| LIPO[Build fat → export as VLDL]
FAST["FASTED state<br/>(glucagon / adrenaline high)"] -->|glycogenolysis| REL[Release glucose from glycogen]
FAST -->|"when glycogen runs low"| GNG["Gluconeogenesis<br/>(make new glucose from<br/>lactate, glycerol, amino acids)"]
REL --> BLOOD[Maintain blood glucose]
GNG --> BLOOD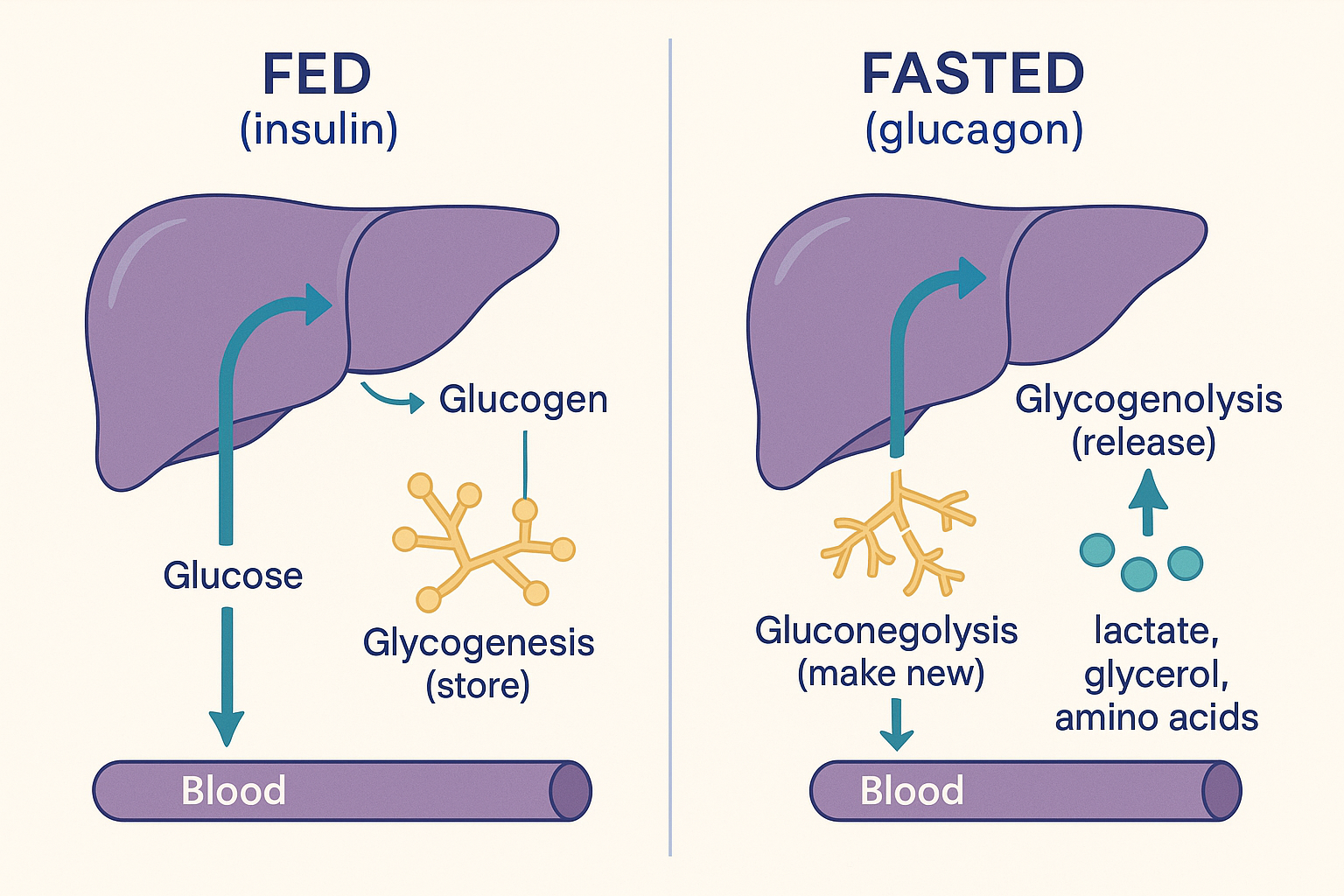 The blood-sugar buffer: store the surplus as glycogen when fed, release it and manufacture more when fasted — so the brain stays supplied either way.
The blood-sugar buffer: store the surplus as glycogen when fed, release it and manufacture more when fasted — so the brain stays supplied either way.
Job 3: Handling fructose — why this sugar is the liver's problem
Here is where a major biohacking talking point becomes clear. The digestion page noted that fructose, like all sugars, is absorbed in the small intestine and travels the portal vein to the liver. The difference is what happens next: the liver metabolises essentially all of it, and it does so in a way that is poorly regulated.
Glucose metabolism is carefully controlled — there is a key regulatory enzyme step (in glycolysis) that slows down when the cell already has enough energy, preventing overload. Fructose skips this control step entirely. It enters the liver's processing pathway below the regulatory gate, via an enzyme called fructokinase that converts it to fructose-1-phosphate without any "are we full?" check. The consequences:
- It rapidly consumes ATP. Phosphorylating fructose uses up the liver cell's ATP (and its phosphate). A large fructose load can transiently deplete liver ATP, which stresses the cell and generates uric acid as a by-product (a link to gout and raised blood pressure).
- It floods the cell with raw carbon with no off-switch. Because there is no regulatory brake, a big fructose load produces a surge of the building-block molecules (DHAP, glyceraldehyde, then acetyl-CoA) that the liver cannot all burn.
- The excess is turned into fat — de novo lipogenesis. "De novo lipogenesis" means making new fat from scratch. The overflow of carbon from heavy fructose intake is converted by the liver into fatty acids. Some is exported as VLDL (raising blood triglycerides), and some accumulates in the liver itself — the mechanistic basis of non-alcoholic fatty liver disease.
This is the precise reason large amounts of fructose (especially from sugar-sweetened drinks, where it arrives fast and in bulk) are implicated in fatty liver and metabolic dysfunction, while the same fructose eaten slowly in whole fruit — buffered by fibre, water, and smaller doses — is far less problematic. It is not that fructose is poison; it is that the liver processes it without a brake, so dose and speed determine whether it overflows into fat.
Job 4: Fat and cholesterol — the liver as lipid hub
The liver is the master control point for fats circulating in your blood. It does several connected things:
- It processes the leftovers of dietary fat. Recall that dietary fat took the lymphatic highway as chylomicrons, bypassing the liver initially. After those chylomicrons drop off most of their fat at tissues, the remnants return to the liver to be dismantled and recycled.
- It packages and exports fat as VLDL. When the liver has surplus fat (from the diet, from de novo lipogenesis, from fructose) it wraps it into particles called VLDL (very-low-density lipoprotein) and ships it out to the body through the blood. VLDL is the precursor of LDL — the "LDL cholesterol" on a blood panel largely originates from this liver export process.
- It synthesises cholesterol. Most of the cholesterol in your body is made by your liver, not eaten — cholesterol is an essential raw material for cell membranes, steroid hormones, and bile. This is also why the cholesterol-lowering statin drugs act on the liver: they block the liver's cholesterol-synthesis enzyme.
- It makes bile acids from cholesterol (see Job 6).
Because the liver both makes, packages, and clears blood fats, its health largely determines your blood lipid profile — far more than dietary cholesterol does.
Job 5: Protein and nitrogen — building blocks and waste disposal
The liver is the body's main protein-handling organ, with two distinct roles:
Building plasma proteins. The liver synthesises most of the critical proteins that circulate in your blood, including:
- Albumin — the most abundant blood protein; it maintains blood volume (by holding water in the vessels) and acts as a transport taxi for fatty acids, hormones, and many drugs. (Recall from the digestion page that fatty acids ride through the blood bound to albumin — the liver makes that albumin.)
- Clotting factors — the proteins that let blood clot; this is why severe liver disease causes bleeding problems.
- Transport proteins — carriers for hormones, iron, and other cargo.
Disposing of nitrogen — the urea cycle. When amino acids are burned for energy or converted to glucose, their nitrogen-containing part must be removed first (a step called deamination). The removed nitrogen becomes ammonia, which is highly toxic — especially to the brain. The liver immediately converts this ammonia into urea, a safe, water-soluble waste molecule, through a series of reactions called the urea cycle. The urea is then sent to the kidneys and excreted in urine. This is why failing livers cause confusion and eventually coma: ammonia is no longer being detoxified into urea and builds up in the blood and brain.
Job 6: Bile — the liver's digestive secretion
We met bile from the receiving end in the digestion page; here is where it is made. Bile is a greenish fluid the liver manufactures from cholesterol. It is stored and concentrated in the gallbladder, and released into the small intestine when fat arrives. Its job, as the digestion page covered, is to emulsify fat — break fat globules into a fine suspension so the enzyme lipase can work and the fat can be absorbed.
The elegant part is the recycling. Bile acids are expensive to make, so the body does not waste them: after they have done their emulsifying work in the upper small intestine, they are reabsorbed in the terminal ileum (the last section of the small intestine), returned via the portal vein to the liver, and reused. This loop is called enterohepatic circulation (gut-liver circulation), and a given pool of bile acids may go around it several times per meal. (This recycling loop is also how the body eliminates some waste products — cholesterol and certain toxins are dumped into bile, and if not reabsorbed, leave in the stool. It is also relevant to how the gut can recirculate things like oestrogen, a theme the gut microbiome page picks up.)
Supplemental bile acids such as TUDCA act within this system, supporting bile flow when it is sluggish.
Job 7: Detoxification — the three-phase disposal system
This is the function people mean when they say "liver detox," and it is far more specific than the wellness-industry usage suggests. The liver neutralises and prepares for excretion a huge range of substances: drugs, alcohol by-products, environmental toxins, and the body's own spent hormones (it is the liver that clears used-up oestrogen, cortisol, and other hormones from circulation). It does this in three sequential phases:
Phase I — transformation (the cytochrome P450 enzymes). A large family of liver enzymes called cytochrome P450 (abbreviated CYP) chemically modify the target molecule — usually by oxidation (adding a reactive oxygen-containing group). This makes the molecule easier to handle in Phase II. Two important wrinkles:
- This is where most drug metabolism happens, and it is why drugs interact. Grapefruit, for instance, blocks a specific CYP enzyme, so drugs cleared by that enzyme build up to higher levels. Different people have genetically different CYP activity, which is why drug responses vary.
- Phase I can make a molecule temporarily more reactive and more toxic, not less. The intermediate it produces often needs Phase II promptly to be made safe. This matters: if Phase I races ahead while Phase II lags (e.g. from nutrient deficiency), reactive intermediates accumulate. (This is exactly what happens with paracetamol/acetaminophen overdose — Phase I produces a toxic intermediate faster than Phase II can neutralise it, and the liver is damaged.)
Phase II — conjugation (making it water-soluble and safe). The liver attaches ("conjugates") a small water-loving molecule onto the Phase I product, which neutralises it and makes it water-soluble so it can be excreted. The main conjugation routes are:
- Glucuronidation — attaching a glucose-derived molecule (the main route for clearing many hormones and drugs; calcium-D-glucarate supports this pathway and the clearance of used oestrogen).
- Sulphation — attaching a sulphate group.
- Glutathione conjugation — attaching glutathione, the body's master antioxidant, which is especially important for neutralising the most reactive and dangerous intermediates. Glutathione is built from the amino acids including cysteine, which is why NAC (N-acetylcysteine) — a cysteine precursor — and glutathione itself are central "liver support" supplements: they keep the most critical Phase II route stocked. (NAC is the actual hospital antidote for paracetamol overdose, precisely because it replenishes the glutathione that the toxic intermediate consumes.)
Phase III — transport out. Dedicated transporter proteins pump the now-safe, water-soluble conjugated molecule out of the liver cell — into the bile (for excretion via the gut) or back into the blood (for excretion via the kidneys).
flowchart LR
TOX["Toxin / drug /<br/>spent hormone<br/>(fat-soluble)"] -->|"Phase I<br/>CYP450 enzymes"| INT["Reactive intermediate<br/>(often MORE toxic)"]
INT -->|"Phase II<br/>conjugation:<br/>glucuronidation · sulphation ·<br/>glutathione"| SAFE["Safe, water-soluble<br/>conjugate"]
SAFE -->|"Phase III<br/>transporters"| OUT["Excreted<br/>via bile or kidneys"]
INT -. "if Phase II lags<br/>→ damage" .-> HARM[Tissue damage]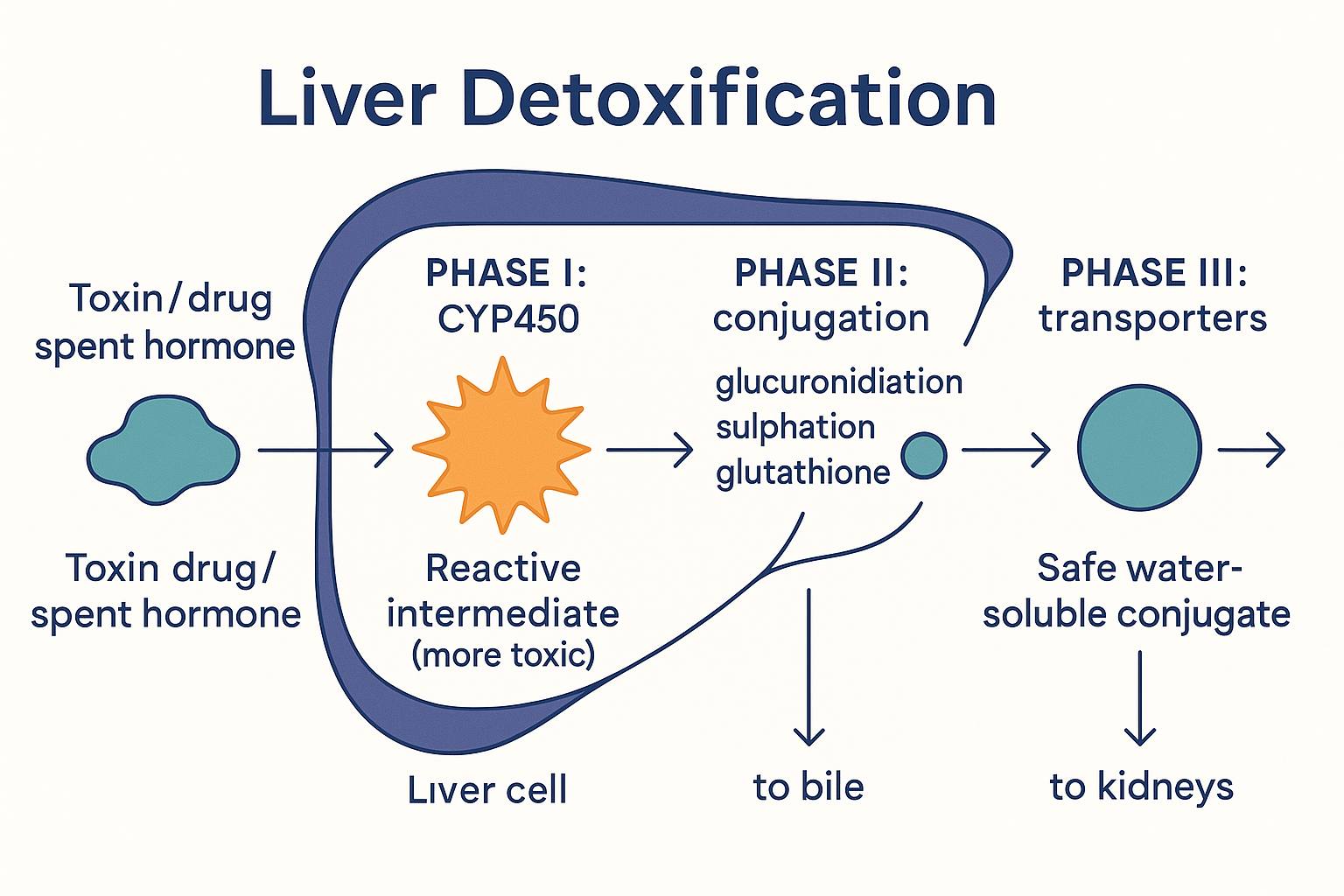 The detox pipeline's hidden danger: Phase I makes the molecule more reactive, so it depends on Phase II keeping up — which is why "liver support" really means stocking the Phase II raw materials like glutathione.
The detox pipeline's hidden danger: Phase I makes the molecule more reactive, so it depends on Phase II keeping up — which is why "liver support" really means stocking the Phase II raw materials like glutathione.
The key engineering insight: detoxification is a two-step pipeline where the intermediate is more dangerous than the input, so Phase I and Phase II must stay balanced. This is why "supporting detox" is really about supplying Phase II raw materials (glutathione, its precursors, the conjugation cofactors) so the pipeline doesn't back up at the dangerous middle stage.
Job 8: Activating thyroid hormone — the liver as the thyroid's partner
This is the liver function fewest people know about, and it connects directly to the next foundations page on metabolism. Your thyroid gland mostly produces T4 (thyroxine) — but T4 is largely a prohormone, a relatively inactive storage form. The active hormone that actually drives your metabolic rate is T3, and most of your T3 is made outside the thyroid, by converting T4 into T3 — and the liver is the primary site where this conversion happens.
The liver performs this conversion using enzymes called deiodinases (specifically type 1, DIO1), which snip one iodine atom off T4 to produce T3. The critical dependencies:
- Selenium is the essential cofactor. The deiodinase enzymes contain selenium; without adequate selenium, the liver cannot efficiently convert T4 to T3. This is a major reason selenium status affects thyroid function.
- The conversion is suppressed by stress and illness. High cortisol (chronic stress), systemic inflammation, fasting, and certain illnesses all blunt the liver's T4→T3 conversion. Under these conditions the liver instead converts T4 into reverse T3 (rT3) — an inactive mirror-image that occupies the system without activating it, effectively a metabolic brake the body applies during hard times.
The consequence is clinically important: you can have perfectly normal T4 blood levels but be functionally low in active T3, because the conversion — a liver job — is impaired. A blood test showing "normal thyroid (T4/TSH)" can therefore miss a real problem that lives in the liver's conversion step. (The full thyroid system, including why the conversion is regulated this way, is the subject of the systemic metabolism page.)
flowchart LR
THY[Thyroid gland] -->|"mostly makes T4<br/>(inactive prohormone)"| T4
T4 -->|"LIVER deiodinase (DIO1)<br/>needs SELENIUM"| T3["T3 (active —<br/>drives metabolism)"]
T4 -.->|"stress, cortisol,<br/>inflammation, fasting"| RT3["reverse T3<br/>(inactive brake)"]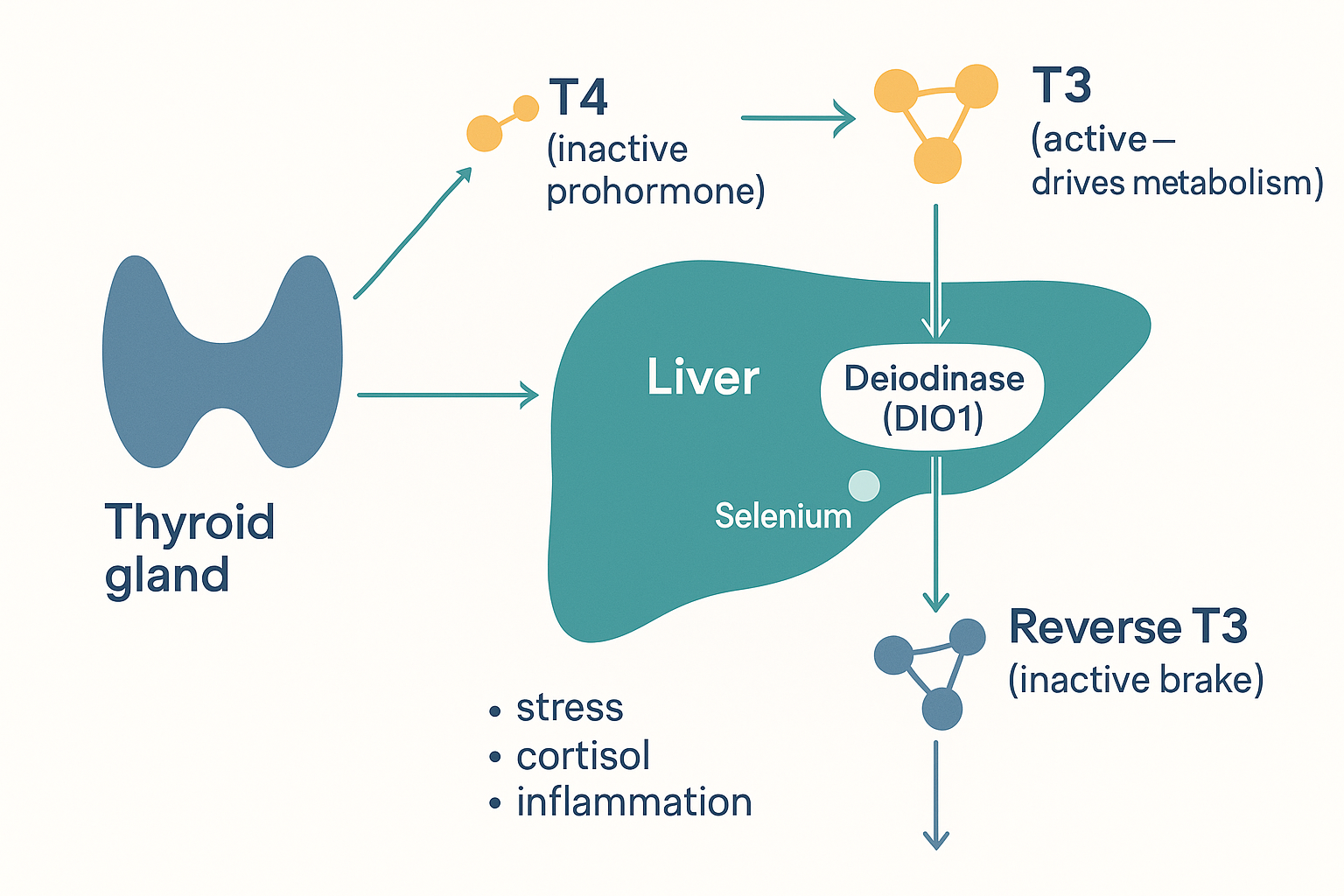 Most active thyroid hormone is made in the liver, not the thyroid: the liver converts inactive T4 into active T3 (needing selenium) — or, under stress, into the inactive reverse-T3 brake.
Most active thyroid hormone is made in the liver, not the thyroid: the liver converts inactive T4 into active T3 (needing selenium) — or, under stress, into the inactive reverse-T3 brake.
Job 9: Alcohol — why the liver pays the price
Alcohol (ethanol) is absorbed quickly, enters the portal vein, and is metabolised almost entirely by the liver — which is why the liver bears the damage from heavy drinking. The pathway is two steps:
- Ethanol → acetaldehyde, by the enzyme alcohol dehydrogenase (ADH). Acetaldehyde is highly toxic — it is responsible for much of the cellular damage and a good part of the hangover. (The flushing reaction many people of East Asian descent experience comes from a genetic variant that makes the next step slow, so acetaldehyde accumulates.)
- Acetaldehyde → acetate, by the enzyme aldehyde dehydrogenase (ALDH). Acetate is relatively harmless and can be used for energy.
But the deeper metabolic problem is a side effect of both steps: they consume enormous amounts of NAD⁺, converting it to NADH. Recall from the cellular energy page that the NAD⁺/NADH ratio is a master regulator — many pathways stall when NAD⁺ runs short. By draining NAD⁺, alcohol metabolism:
- Blocks fat oxidation — the liver can't burn fat when NAD⁺ is depleted, so fat accumulates (the first stage of alcoholic fatty liver, which can appear after even a single heavy session).
- Blocks gluconeogenesis — the liver can't make new glucose, which is why heavy drinking on an empty stomach can cause dangerous hypoglycaemia.
- Pushes lactate up — contributing to acidosis and raised uric acid.
So alcohol doesn't just deliver a toxin (acetaldehyde); it hijacks the liver's core redox currency (NAD⁺), paralysing several of the other jobs on this page at once. It is a clean illustration of how interconnected the liver's functions are — disrupt one shared resource and many systems falter together.
Putting it all together
The liver sits at the crossroads of everything you absorb and everything your cells need:
- Position: two inflow pipes (portal vein with nutrients, hepatic artery with oxygen), one outflow to blood (hepatic vein), one outflow to gut (bile). Everything water-soluble you absorb passes through here first.
- Blood sugar: stores surplus glucose as glycogen (insulin) and releases it (glucagon/adrenaline); makes new glucose from scratch (gluconeogenesis) when stores run low — keeping the brain supplied with or without carbs.
- Fructose: processes it without a regulatory brake, so large fast loads overflow into liver fat (de novo lipogenesis → fatty liver).
- Fat: processes chylomicron remnants, exports fat as VLDL, makes most of the body's cholesterol, and turns cholesterol into bile.
- Protein: builds albumin and clotting factors; disposes of amino-acid nitrogen as urea (protecting the brain from ammonia).
- Bile: made from cholesterol, recycled via enterohepatic circulation, essential for fat absorption.
- Detox: a three-phase pipeline (CYP450 transform → conjugation → transport out) where the middle intermediate is the most dangerous, so Phase II raw materials like glutathione are what "support" really means.
- Thyroid: converts inactive T4 into active T3 (needs selenium; blunted by stress) — so metabolic rate partly depends on liver health.
- Alcohol: detoxified here at the cost of draining NAD⁺, which simultaneously stalls fat-burning and glucose-making.
The unifying idea: the liver is a buffer and a transformer. It smooths out the feast-and-famine of eating (storing and releasing fuel), and it chemically converts raw or dangerous molecules into useful or safe ones. When people talk about "liver support," what they are really talking about is supplying the raw materials — glutathione precursors, conjugation cofactors, selenium, bile support — that these transformations depend on.
Related Compounds & Deep Dives
Detoxification support (Phase II raw materials)
- NAC (N-acetylcysteine) — cysteine precursor for glutathione; the clinical antidote for paracetamol overdose, which works by replenishing the glutathione that Phase II depends on.
- Glutathione — the master antioxidant and the key Phase II conjugation molecule for the most reactive intermediates.
- Calcium-D-glucarate — supports the glucuronidation pathway and the clearance of spent oestrogen.
- Glycine and taurine — amino acids used in Phase II conjugation and in bile acid formation.
Bile & fat handling
- TUDCA — a bile acid that supports bile flow within the enterohepatic circulation.
- Choline, betaine, inositol — "lipotropic" factors that help the liver export fat (as VLDL) and resist fatty accumulation.
- Coconut oil / MCTs — medium-chain fats that arrive at the liver via the portal vein and are rapidly burned or made into ketones.
Thyroid conversion
- Selenium — essential cofactor for the deiodinase enzymes that convert T4 to T3 in the liver.
- T4 and T3 — the prohormone and the active hormone the liver's conversion step connects.
Blood-sugar & fuel signalling
- Insulin — drives the liver to store glucose as glycogen and to build fat.
- Cortisol — drives gluconeogenesis and blunts the liver's T4→T3 conversion.
- Glucose — the fuel the liver buffers via glycogen and manufactures via gluconeogenesis.
Antioxidant / protective
Related foundations
- Digestion — how material reaches the liver via the portal vein in the first place.
- Cellular Energy — what the fuels the liver dispatches are used for in the cell; the NAD⁺ currency that alcohol drains.
- Systemic Metabolism — the full thyroid and hormonal system the liver's T4→T3 conversion feeds into.