Magnesium
The mineral that every ATP molecule depends on — and why the form determines whether it reaches your brain, your muscles, or your gut.
Why magnesium is different from most minerals
Most minerals are cofactors — they help enzymes work. Magnesium is that, but at a scale nothing else matches: it's a required cofactor for over 300 enzyme systems, and it has a second, more fundamental role that most people miss.
ATP does not exist in cells as ATP. It exists as Mg-ATP.
The magnesium ion binds to the phosphate groups of ATP and stabilises the molecule. Without Mg²⁺, ATP cannot be recognised or used by the enzymes that consume it — kinases, ATPases, ATP synthase itself. Every time a cell makes or uses energy, it needs magnesium. This means deficiency doesn't just affect one pathway — it creates a low-level failure across every energy-dependent process simultaneously.
The second fundamental role is at the NMDA receptor, which governs learning and memory. That mechanism is covered in the L-Threonate section below.
Why deficiency is widespread
Estimated 45–50% of the US population consumes less than the Estimated Average Requirement for magnesium. In the UK the picture is similar. Several factors compound this:
- Soil depletion — industrial agriculture has progressively reduced mineral content in topsoil. Magnesium levels in vegetables have declined 20–30% since the 1950s.
- Food processing — refining grains removes the bran and germ where magnesium concentrates. White bread retains ~20% of the magnesium in wholegrain.
- High sugar / refined carb intake — glucose metabolism increases urinary magnesium excretion. High-carb diets actively deplete magnesium.
- Alcohol — increases urinary excretion and reduces intestinal absorption.
- Proton pump inhibitors — reduce gastric acid, which impairs magnesium absorption; long-term PPI use causes clinical hypomagnesaemia.
- High stress — cortisol increases renal magnesium excretion; magnesium is consumed by adrenal function.
- Intense exercise — sweat losses plus metabolic demand during high-output exercise significantly depletes magnesium.
Standard serum magnesium tests are unreliable for detecting insufficiency. Only ~1% of total body magnesium is in serum; the rest is intracellular and in bone. Serum levels are tightly regulated and fall only late. A "normal" serum level is compatible with significant intracellular depletion.
What magnesium does — the key mechanisms
Mg-ATP: the energy substrate
Every enzyme that uses ATP as a substrate is actually using Mg-ATP. This includes: - DNA and RNA polymerases — cell replication and repair - All kinases — phosphorylation signalling cascades - Na⁺/K⁺-ATPase — maintains membrane potential in every cell - Ca²⁺-ATPase — pumps calcium out of cells after contraction - ATP synthase — synthesises ATP in mitochondria
Subclinical magnesium deficiency creates a state where all these processes are running at reduced capacity. The clinical picture — fatigue, brain fog, muscle tension, poor sleep, anxiety — maps precisely onto what happens when ATP utilisation is broadly impaired.
NMDA receptor block — why Mg is a brain mineral
The NMDA receptor is the molecular switch for synaptic plasticity — the cellular mechanism of learning and memory. At resting membrane potential, a Mg²⁺ ion sits inside the channel pore and physically blocks calcium from entering.
This block is voltage-dependent: when the membrane depolarises sufficiently (because the glutamate-sensitive AMPA receptor is activated at the same time), the Mg²⁺ is expelled and Ca²⁺ can flow through. The NMDA receptor therefore acts as a coincidence detector — it only opens when two things happen simultaneously: ligand binding AND sufficient depolarisation.
This is the molecular basis of Hebbian plasticity ("neurons that fire together, wire together"). Long-term potentiation (LTP), the cellular correlate of memory formation, requires NMDA receptor activation.
How does Mg deficiency affect this? Paradoxically, lower intracellular Mg weakens the block, which sounds like it would improve signalling. But a weak block means the receptor opens too easily — random background noise gets through along with meaningful signals. Signal-to-noise ratio collapses. The result is not enhanced memory but degraded synaptic specificity: everything is slightly activated, nothing is strongly potentiated. Anxiety, hyperreactivity, and brain fog follow.
Restoring adequate Mg strengthens the block, which allows the receptor to function as a proper coincidence detector again — strong, specific signals break through, weak noise doesn't.
flowchart TD
REST["Resting neuron<br/>(no strong input)"] --> PLUG["Mg²⁺ sits in the NMDA channel pore<br/>→ blocks Ca²⁺ entry"]
PLUG --> NOISE["Random weak signals bounce off<br/>(noise filtered out)"]
COINC["Glutamate binds AND<br/>membrane depolarises (AMPA fires)"] --> EXPEL["Mg²⁺ expelled from pore"]
EXPEL --> CA["Ca²⁺ floods in"]
CA --> LTP["LTP — the memory is written<br/>(only for strong, coincident signals)"]
LOWMG["Low Mg → weak block"] -. "everything leaks through<br/>→ noise, anxiety, poor specificity" .-> NOISE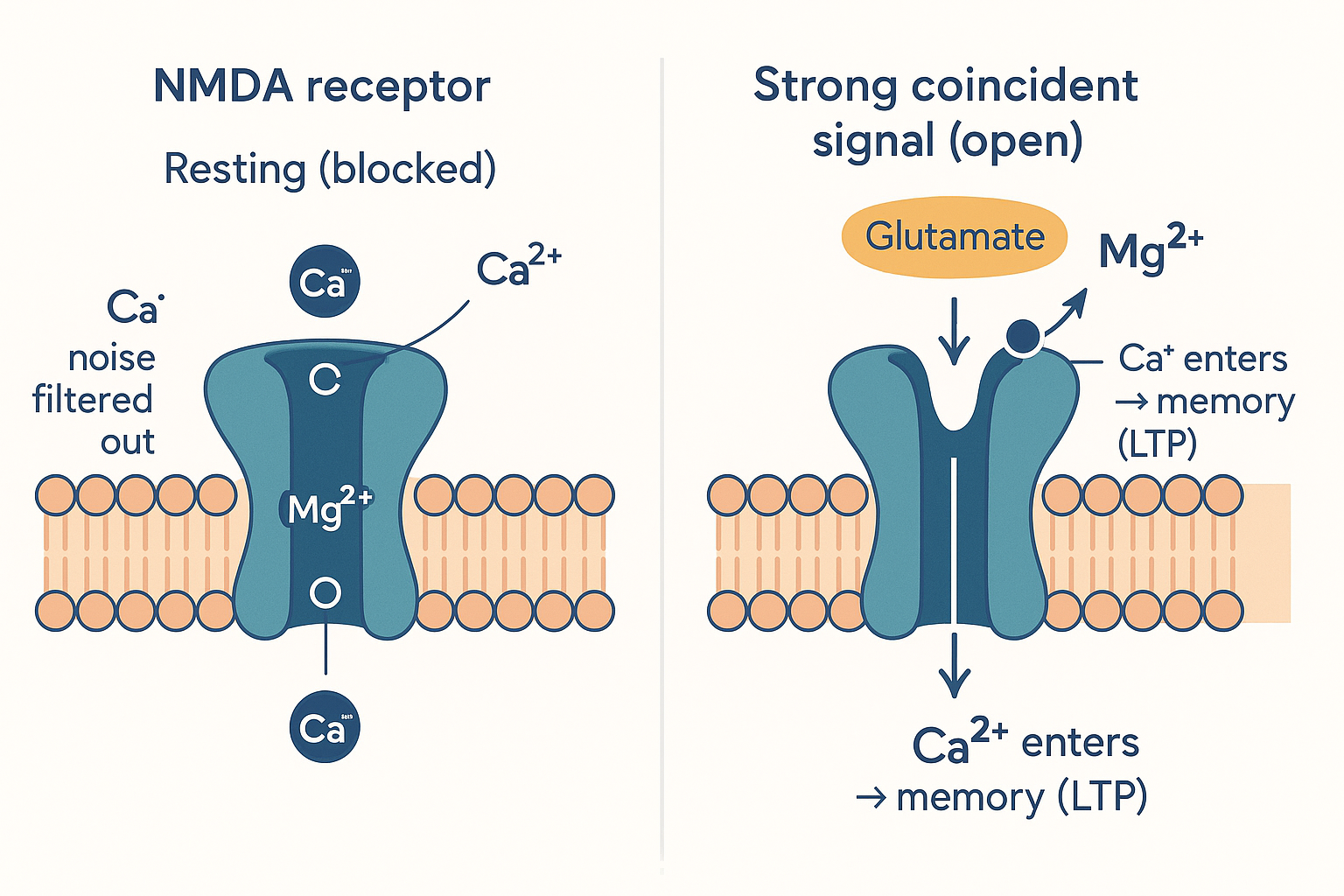 The coincidence detector: Mg²⁺ plugs the pore and filters out weak noise; only a strong, coincident signal expels it and lets Ca²⁺ in to write the memory.
The coincidence detector: Mg²⁺ plugs the pore and filters out weak noise; only a strong, coincident signal expels it and lets Ca²⁺ in to write the memory.
Muscle relaxation (Ca/Mg antagonism)
Calcium triggers muscle contraction; magnesium drives relaxation. Mg²⁺ competes with Ca²⁺ for binding sites on contractile proteins and blocks voltage-gated calcium channels. Deficiency shifts the balance toward sustained contraction — muscle cramps, tension, twitching, restless legs.
HPA axis and cortisol regulation
Magnesium directly suppresses the hypothalamic-pituitary-adrenal axis at multiple points. It reduces CRH secretion from the hypothalamus and blunts adrenal sensitivity to ACTH. Deficiency leads to HPA overactivation — chronically elevated cortisol, which in turn increases urinary Mg loss. This creates a self-reinforcing cycle: stress depletes Mg, low Mg amplifies the stress response.
The forms — why it matters enormously
Magnesium supplements vary dramatically in bioavailability, tissue targeting, and secondary effects. The anion (the molecule it's bound to) determines all three.
flowchart LR
OX["Oxide<br/>~4% absorbed"] --> GUT["Stays in gut<br/>→ laxative only"]
CIT["Citrate<br/>~25–30%"] --> GUT2["Gut + mild laxative<br/>→ constipation, migraine"]
GLY["Glycinate / bisglycinate<br/>~80%"] --> SLEEP["Body + calm<br/>→ sleep, anxiety, muscle"]
THR["L-Threonate"] -->|"crosses BBB via SVCT2"| BRAIN["Brain<br/>→ cognition, memory"]Magnesium Oxide — avoid for supplementation
Bioavailability: ~4%
The most common form in cheap multivitamins and labelled "500 mg magnesium" on packaging. The oxide anion does not chelate the Mg²⁺ — it simply holds it in a salt. Almost entirely excreted. What little reaches the gut draws water osmotically into the lumen and acts as a laxative. Not appropriate for repleting magnesium status.
Magnesium Citrate — useful for gut
Bioavailability: ~25–30%
Water-soluble, reasonably well absorbed, and retains a mild osmotic laxative effect. The citrate anion enters the Krebs cycle. Best use case: addressing constipation alongside mild magnesium insufficiency. The laxative effect is dose-dependent — at 200–300 mg elemental Mg, most people see softened stools without frank diarrhea.
Not optimal for sleep or cognitive goals because there's no specific tissue targeting.
Magnesium Glycinate / Bisglycinate — the sleep and anxiety form
Bioavailability: ~80%+ (chelated)
Magnesium glycinate is magnesium chelated to glycine — the Mg²⁺ ion is bound inside the glycine molecule's coordination sphere rather than held as a salt. This has two consequences:
1. Superior absorption. Chelated minerals use amino acid transporters (PepT1, PepT2) rather than the mineral-specific divalent metal transporters, which are lower-capacity and subject to competition from calcium, zinc, and iron. Chelated Mg bypasses this competition and is absorbed intact across the intestinal epithelium, then cleaved inside enterocytes.
2. You're also dosing glycine. Glycine is a major inhibitory neurotransmitter in the spinal cord and brainstem (acting on strychnine-sensitive glycine receptors). It is also a co-agonist at NMDA receptors (the GluN1 glycine-binding site). Systemically, glycine lowers core body temperature — a critical trigger for sleep onset — and independently improves sleep quality, reducing sleep latency and improving slow-wave sleep even at 3g/day.
The combined effect of Mg (muscle relaxation, HPA suppression) and glycine (temperature drop, inhibitory tone, NMDA modulation) makes magnesium glycinate the optimal form for sleep and anxiety.
Typical dose: 200–400 mg elemental Mg as glycinate (= 1–2g of magnesium glycinate salt), taken 30–60 min before sleep.
Practical note: "Bisglycinate" means two glycine molecules per Mg²⁺ ion — it's the same compound, more completely chelated. Prefer bisglycinate where available.
Magnesium L-Threonate — the brain form
Bioavailability: moderate systemically, uniquely high in CNS
This is the most mechanistically interesting form and requires separate treatment.
Origin
Developed by a team led by Guosong Liu at MIT (now Tsinghua University). The key insight: all other forms of magnesium raise blood and peripheral tissue levels, but brain magnesium is separately regulated and is notoriously hard to increase through supplementation. The BBB tightly controls Mg transport into the CNS, and inorganic or simple organic Mg forms don't cross efficiently enough to raise intracellular brain concentrations meaningfully.
L-Threonate is a natural metabolite of Vitamin C (ascorbic acid). The threonate anion has a specific affinity for the SVCT2 transporter (sodium-dependent vitamin C transporter 2), which is highly expressed in the choroid plexus and neurons. Binding to this transporter allows the Mg-threonate complex to be actively transported into the CNS rather than relying on passive diffusion.
The landmark study (Slutsky et al., 2010, Neuron)
Rats supplemented with Mg-threonate showed: - Significantly elevated hippocampal and cortical Mg²⁺ levels (other Mg forms did not) - Increased synaptic density in hippocampal neurons — specifically in CA1 and CA3 - Improved short-term memory (novel object recognition) - Improved long-term memory (contextual fear conditioning) - Enhanced LTP — the Mg²⁺ block was stronger and more precise, improving signal-to-noise in NMDA-dependent plasticity
The mechanism: more intracellular Mg in neurons → stronger NMDA voltage-dependent block → better coincidence detection → more specific LTP → improved learning and memory consolidation.
Human evidence
Human RCTs are smaller than ideal but directionally consistent. Studies using 1.5–2g/day of Mg-threonate (delivering ~144 mg elemental Mg) have shown improvements in: - Cognitive flexibility and executive function in middle-aged and older adults - Sleep quality (brain Mg independently regulates sleep architecture) - Anxiety reduction (the NMDA modulation angle)
One placebo-controlled crossover found significant improvement on the Trail Making Test and Stroop task in adults over 50 after 12 weeks.
Dosing
The original Magtein product (licensed from MIT) is standardised to deliver 144 mg elemental Mg per 3-capsule serving. This is a lower elemental dose than glycinate but the CNS bioavailability is what matters.
Timing: morning or early afternoon — raises alertness and cognitive performance, not sedating. Some users take glycinate at night and threonate in the morning.
Note: Mg-threonate should not be your only magnesium source. The 144 mg elemental dose doesn't substantially move whole-body Mg status. Stack it with glycinate for comprehensive coverage.
Other forms — brief
| Form | Bioavailability | Best for | Notes |
|---|---|---|---|
| Malate | ~60% | Fatigue, fibromyalgia | Malate is a Krebs cycle intermediate; synergy with energy production |
| Taurate | Moderate | Cardiovascular, insulin sensitivity | Taurine has independent cardiac and metabolic benefits |
| Chloride | ~60% | Transdermal or oral | Epsom salts = magnesium sulfate (mostly absorbed transdermally? — evidence is weak) |
| Orotate | Moderate | Heart failure, athletic performance | Orotic acid facilitates Mg into cardiac cells; used in German cardiology |
| Threonate | Unique (brain) | Cognition, learning, memory | See above |
| Glycinate | ~80% | Sleep, anxiety, muscle | See above |
Magnesium and sleep — the full picture
Sleep is where magnesium effects are most reliably felt. Three mechanisms converge:
1. NMDA receptor modulation in sleep centres. The suprachiasmatic nucleus (circadian master clock) and ventrolateral preoptic area (sleep switch) are both NMDA-rich. Adequate Mg stabilises these circuits.
2. GABA potentiation. Mg²⁺ enhances GABA-A receptor activity — the same receptor class targeted by benzodiazepines, but via a distinct, non-addictive mechanism. This increases inhibitory tone in the brain at sleep onset.
3. Cortisol suppression. By blunting HPA axis activity, Mg reduces night-time cortisol — the stress hormone that causes middle-of-the-night waking and fragmented sleep architecture.
A 2012 RCT in elderly adults with insomnia (PMID 23853635) showed magnesium supplementation (500 mg/day, 8 weeks) significantly improved sleep onset, total sleep time, sleep efficiency, and early morning waking compared to placebo. Serum cortisol decreased, serum melatonin increased.
Magnesium and migraine
Neurological Mg deficiency is well-documented in migraine sufferers — cortical spreading depression (the wave of depolarisation underlying migraine aura) is more easily triggered in low-Mg states. The American Academy of Neurology includes magnesium in its migraine prophylaxis guidelines (Level B evidence — probably effective).
Dose for migraine prevention: 400–600 mg elemental Mg/day (citrate or glycinate). IV magnesium sulfate is used acutely in emergency settings for status migrainosus.
Practical approach
For sleep and recovery (most common use case): → Magnesium glycinate or bisglycinate, 200–400 mg elemental Mg, 30–60 min before bed
For cognitive performance and learning: → Magnesium L-Threonate (Magtein), 3 caps/day (144 mg elemental), morning
For comprehensive coverage: → Both: threonate in the morning, glycinate at night
For migraine prevention: → Magnesium citrate or glycinate, 400–600 mg/day
For gut/constipation: → Magnesium citrate, 200–400 mg at night
Avoid: magnesium oxide for anything other than acute constipation. Avoid at pharmacological doses alongside tetracycline or fluoroquinolone antibiotics (Mg chelates and inactivates them).
Cofactors
Magnesium status interacts with: - Vitamin D — Mg is required to activate vitamin D (both conversion steps: 25-hydroxylation and 1-alpha hydroxylation). Supplementing high-dose D3 without adequate Mg can deplete Mg rapidly. - Vitamin B6 — synergistic in reducing anxiety and PMS symptoms in RCTs; B6 increases intracellular Mg uptake. - Potassium — Mg deficiency causes renal potassium wasting; refractory hypokalaemia often resolves only when Mg is repleted first. - Calcium — Ca:Mg ratio matters. High-dose calcium supplementation without corresponding Mg shifts the balance toward vasoconstriction and muscle tension.
UK sourcing
| Product | Form | Notes |
|---|---|---|
| Thorne Magnesium Bisglycinate | Bisglycinate | Clean formulation, well-dosed |
| Bulk Magnesium Bisglycinate | Bisglycinate | Budget-friendly, available in powder form for flexible dosing |
| Magtein (various UK stockists) | L-Threonate | Licensed Slutsky/Liu formulation — specify Magtein brand to ensure genuine patent |
| Now Foods Magnesium Glycinate | Glycinate 100 mg | Widely available, cost-effective |
| Viridian Magnesium Citrate | Citrate | UK brand, good for constipation/migraine angle |
Research sources
- PMID 20152124 — Slutsky I et al. (2010). Enhancement of learning and memory by elevating brain magnesium. Neuron 65(2):165–177. Founding Mg-threonate paper: rats, hippocampal Mg, synaptic density, LTP, short- and long-term memory.
- PMID 36558392 — Zhang C et al. (2022). A Magtein®-based formula improves brain cognitive functions in healthy Chinese adults. Nutrients 14(24):5235. Double-blind RCT, n=102, 30 days — Memory Quotient improved significantly. Caveat: multi-ingredient formula, not pure MgT.
- PMID 33865376 — Mah J & Pitre T (2021). Oral magnesium supplementation for insomnia in older adults: systematic review & meta-analysis. BMC Complement Med Ther 21:125. 3 RCTs: sleep onset latency −17 min vs placebo (p=0.0006); evidence quality low–very low.
- PMID 28445426 — Boyle NB et al. (2017). The effects of magnesium supplementation on subjective anxiety and stress. Nutrients 9(5):429. Systematic review: positive anxiety effects in mildly anxious and PMS populations; overall evidence quality poor.
- PMID 21835188 — Sartori SB et al. (2012). Magnesium deficiency induces anxiety and HPA axis dysregulation. Neuropharmacology 62(1):304–12. Animal study: dietary Mg restriction elevated CRH, ACTH, and anxiety behaviour.
- PMID 29387426 — DiNicolantonio JJ et al. (2018). Subclinical magnesium deficiency: a principal driver of cardiovascular disease and a public health crisis. Open Heart 5(1):e000668. ~50% Americans below EAR; historical food content losses documented.
- PMID 8792038 — Peikert A et al. (1996). Prophylaxis of migraine with oral magnesium: multi-centre RCT. Cephalalgia 16(4):257–63. n=81; 600 mg/day, 12 weeks; attack frequency −41.6% vs −15.8% placebo (p<0.05).
- PMID 22293292 — Bannai M & Kawai N (2012). Glycine improves the quality of sleep. J Pharmacol Sci 118(2):145–8. Oral glycine lowered core body temperature via cutaneous vasodilation; improved sleep quality.
- PMID 25533534 — Kawai N et al. (2015). Sleep-promoting and hypothermic effects of glycine are mediated by NMDA receptors in the SCN. Neuropsychopharmacology 40(6):1405–16. SCN ablation abolished glycine-induced sleep promotion; NMDA antagonists blocked temperature drop.
- PMID 6325946 — Mayer ML, Westbrook GL, Guthrie PB (1984). Voltage-dependent block by Mg²⁺ of NMDA responses in spinal cord neurones. Nature 309:261–3. Established physiological Mg block of NMDA channels at resting potential.
- PMID 6320006 — Nowak L et al. (1984). Magnesium gates glutamate-activated channels in mouse central neurones. Nature 307:462–5. Independent concurrent confirmation of voltage-dependent Mg gating.
- PMID 14596323 — Walker AF et al. (2003). Mg citrate found more bioavailable than other Mg preparations. Magnes Res 16(3):183–91. n=46; hierarchy: citrate > chelate > oxide; oxide not different from placebo.
- PMID 2407766 — Lindberg JS et al. (1990). Magnesium bioavailability from magnesium citrate and magnesium oxide. J Am Coll Nutr 9(1):48–55. MgO virtually insoluble; citrate dramatically higher urinary recovery.