Digestion: From Mouth to Cell
The complete journey of everything you swallow — food, supplements, drugs — from the moment it enters your mouth to the moment its molecules reach the cells that use them. Where each thing is absorbed, why there, and which route it takes through the body.
Why this page exists
People hear contradictory things about digestion all the time. "Take it sublingually so it bypasses the liver." "Fructose goes straight to the liver." "Fat is absorbed differently." "Coconut oil is special." "Take this on an empty stomach, that one with food." Almost all of these statements are true — but they only make sense once you understand the actual plumbing.
This page lays out that plumbing as a single continuous journey. We follow what you swallow down the entire tract, stopping at each organ to ask three engineer's questions: what gets broken down here, what gets absorbed here, and where does it go next? By the end you should be able to predict, for almost any molecule, where it will be absorbed and which route it will travel.
One organising idea makes the whole page click, so we introduce it first.
The single most important concept: two different highways out of the gut
When a molecule is absorbed from your gut, it does not just "enter the blood" as one undifferentiated event. There are two completely separate exit routes, and which one a molecule takes determines what happens to it next:
-
The portal vein highway. Most absorbed molecules — sugars, amino acids, water-soluble vitamins, most drugs, alcohol — enter small blood vessels in the gut wall that all drain into one large vessel called the hepatic portal vein. This vein does not go to the general circulation. It goes directly to the liver first. Everything on this highway is inspected and processed by the liver before it ever reaches the rest of your body. This mandatory liver checkpoint is called first-pass metabolism, and it is one of the most important concepts in all of physiology and pharmacology.
-
The lymphatic highway. Dietary fat is the great exception. Absorbed fat is too bulky and fat-soluble to travel in blood directly, so it is packaged into particles and routed into the lymphatic system — a separate network of vessels that drains, eventually, into a large vein near the heart (the subclavian vein). Crucially, this route bypasses the liver's first-pass checkpoint and dumps its cargo straight into the general circulation. The liver gets its turn later, on a second lap.
Hold these two highways in your mind for the entire page. Nearly every "why is this absorbed differently?" question reduces to: which highway does it take, and does it pass through the liver first or not?
flowchart TD
GUT[Molecule absorbed from gut wall]
GUT --> Q{Water-soluble<br/>or fat?}
Q -->|"sugars, amino acids,<br/>water-soluble vitamins,<br/>most drugs, alcohol"| PV[Hepatic portal vein]
Q -->|"dietary fat,<br/>fat-soluble vitamins A D E K"| LYMPH[Lymphatic system]
PV --> LIVER["LIVER<br/>(first-pass metabolism —<br/>inspected & processed here first)"]
LIVER --> SYS[General circulation → body]
LYMPH --> SYS2[General circulation → body<br/>liver gets a turn later]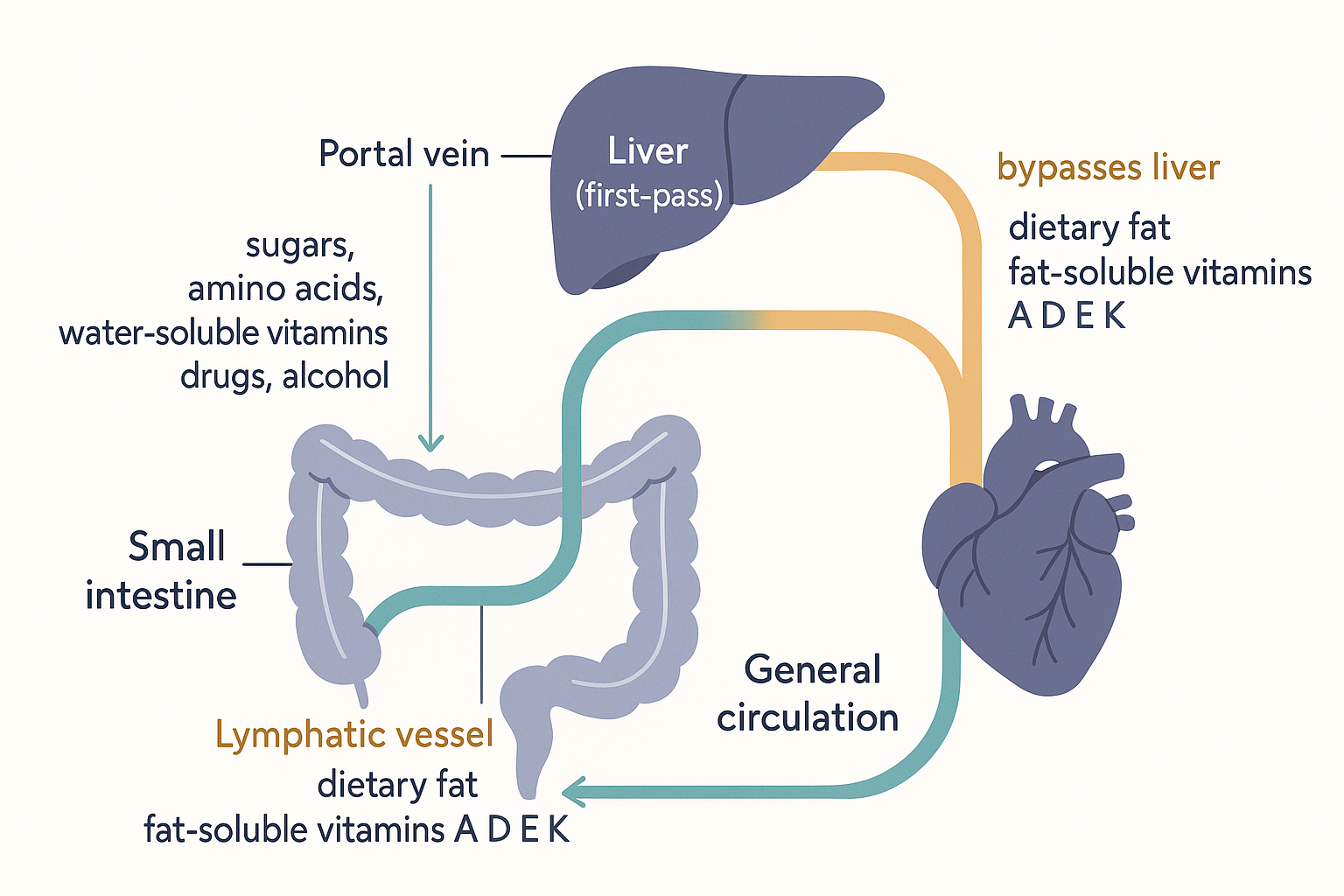 The two highways out of the gut: the portal route (teal) is forced through the liver's first-pass checkpoint; the lymphatic route (amber) goes around it.
The two highways out of the gut: the portal route (teal) is forced through the liver's first-pass checkpoint; the lymphatic route (amber) goes around it.
There is also a third way to reach the blood that skips the gut entirely — absorbing a molecule across a mucous membrane before it is ever swallowed. That is the sublingual route, and we cover it below. But for anything you actually swallow, it is one of the two highways above.
Here is the whole tract at a glance — the stops we are about to walk through, and what each one does:
flowchart TD
M["MOUTH<br/>chew · salivary amylase (starch)<br/>sublingual bypass possible"] --> O[Oesophagus<br/>just a pipe]
O --> S["STOMACH<br/>acid + pepsin denature protein<br/>sets gastric emptying pace<br/>absorbs: alcohol, a few drugs"]
S --> SI["SMALL INTESTINE<br/>★ main absorption site ★<br/>bile + pancreatic enzymes<br/>carbs · protein · fat · vitamins"]
SI --> LI["LARGE INTESTINE / COLON<br/>water reabsorbed<br/>bacteria ferment fibre → SCFAs<br/>rectal bypass possible"]
LI --> ST[Stool]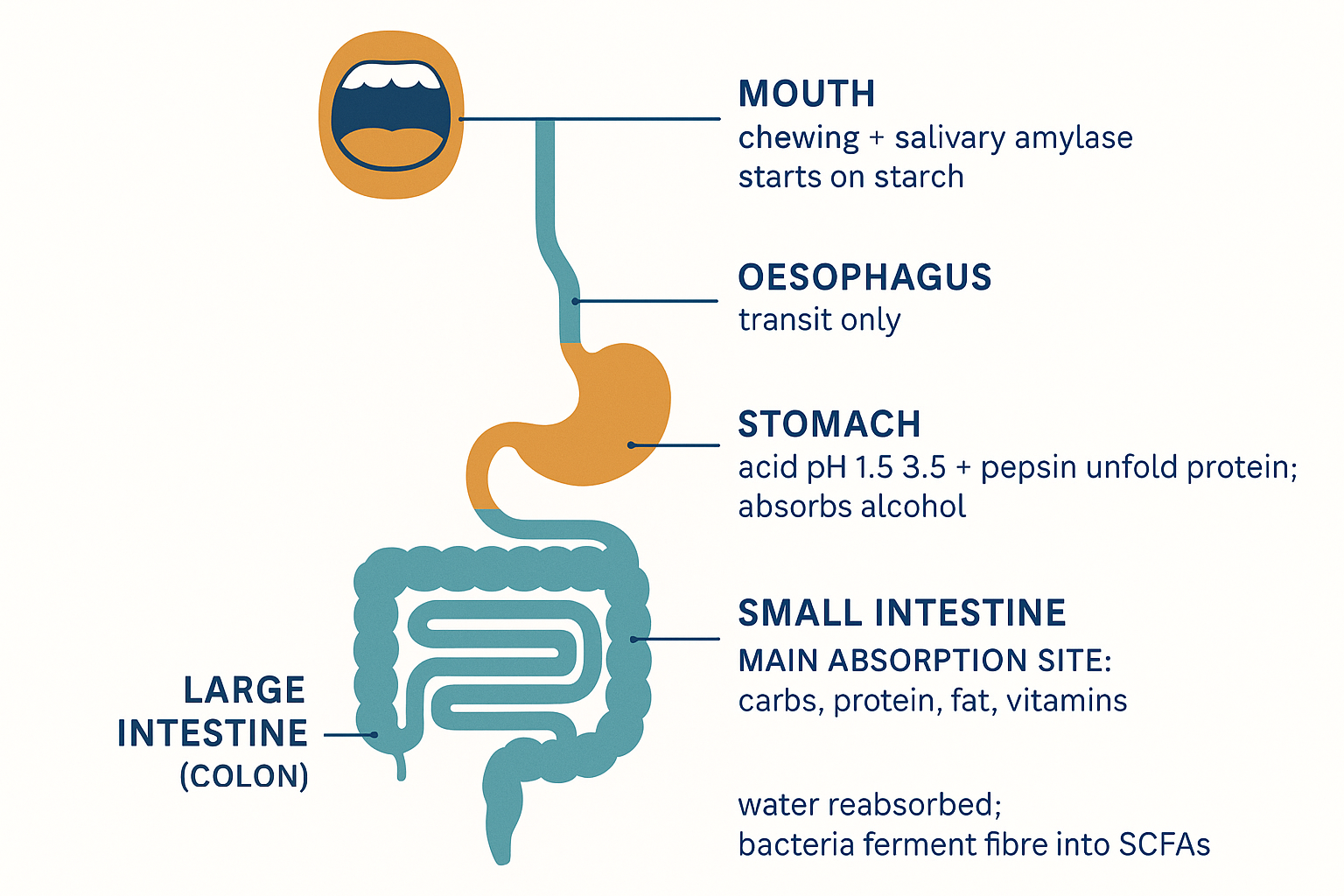 The tract as a sequence of stations — each one prepares, breaks down, or absorbs, and the small intestine does most of the absorbing.
The tract as a sequence of stations — each one prepares, breaks down, or absorbs, and the small intestine does most of the absorbing.
Stop 1: The mouth — mechanical breakdown begins, plus one chemical head-start
Digestion starts before you swallow. Two things happen in the mouth:
-
Mechanical breakdown. Chewing physically shreds food into smaller pieces, massively increasing the surface area that enzymes can later work on. This sounds trivial but it is rate-limiting: poorly chewed food is digested slower and less completely downstream.
-
Salivary amylase. Saliva contains an enzyme called amylase (specifically salivary amylase, also called ptyalin) that begins breaking down starch — long chains of glucose — into shorter sugar fragments. This is why a piece of plain bread starts to taste faintly sweet if you hold it in your mouth: amylase is liberating glucose. (This enzyme is then mostly shut down by stomach acid moments later, so it only gets a brief head-start.)
Very little is actually absorbed in the mouth during normal eating — food does not linger long enough. The mouth's job is preparation, not absorption. But there is one important exception, and it is deliberately exploited.
Stop 1b: Sublingual absorption — the deliberate liver bypass
The tissue under the tongue (and inside the cheek) is thin, and right beneath it sits a dense bed of blood vessels. If a molecule is held there long enough and has the right properties, it can be absorbed directly across that mucous membrane into the bloodstream — without being swallowed, without passing through the stomach or gut, and critically without first-pass metabolism by the liver. This is the sublingual (under-the-tongue) route.
Why would you want to bypass the liver? Because the liver's first-pass checkpoint can destroy a large fraction of certain molecules before they ever reach the body. If a drug or hormone is heavily broken down on first pass, swallowing it wastes most of the dose. Taking it sublingually delivers far more of it intact. This is why some hormones (e.g. certain forms of progesterone, testosterone), certain B12 preparations, and drugs like nitroglycerin (for chest pain, where speed also matters) are taken sublingually.
Not everything can be absorbed this way. To cross the mouth lining efficiently, a molecule generally needs to be:
- Fat-soluble (lipophilic) enough to slip through the fatty cell membranes of the mucosa — strongly water-loving molecules struggle.
- Small enough — large molecules (most proteins and peptides) do not cross well.
- Potent at a low dose — only a small amount of material can dissolve and absorb under the tongue, so the substance has to be effective in milligram or microgram quantities. You cannot meaningfully take grams of something sublingually.
- Stable at the mouth's near-neutral pH.
Does it work with food, or only powders/tablets? It is fundamentally a property of the molecule and contact time, not the format. It works with a tablet, a drop of liquid, or a powder held under the tongue — anything that lets the substance dissolve in saliva and sit against the mucosa long enough. It does not work if you immediately chew and swallow, because then it just enters the normal digestive tract. The key is sustained contact with the mucous membrane.
Stop 2: The oesophagus — just a pipe
The oesophagus is the muscular tube connecting throat to stomach. It absorbs essentially nothing; its only job is to move the swallowed bolus downward by waves of muscle contraction (peristalsis — the coordinated squeeze that propels contents along the entire gut). We mention it only to be complete: nothing of metabolic interest happens here.
Stop 3: The stomach — acid, protein unfolding, and a gatekeeper
The stomach is a muscular, acidic mixing chamber. Three things define it:
The acid environment. The stomach lining secretes hydrochloric acid, bringing the contents to a strongly acidic pH of roughly 1.5–3.5 (pH is the scale of acidity; lower means more acidic; pure water is 7). This acid does several jobs at once: it kills most swallowed bacteria, it unfolds proteins, and it activates the stomach's main digestive enzyme.
Protein denaturation and pepsin. Proteins are long chains folded into tight 3D shapes. The acid denatures them — unravels the folds — exposing the chain so enzymes can cut it. The stomach secretes an inactive enzyme precursor called pepsinogen, which the acid converts into the active enzyme pepsin. Pepsin begins chopping proteins into shorter fragments (peptides). Note the dependency: no acid → no active pepsin → poor protein breakdown. This is the mechanistic basis for taking betaine HCl or apple cider vinegar with protein-heavy meals — they lower stomach pH to support pepsin activation in people with low stomach acid.
It is mostly a holding and mixing tank, not an absorption site. Surprisingly little is absorbed across the stomach wall, because the stomach lining is built to resist its own acid, not to absorb nutrients. A few small, fat-soluble molecules do get through here: alcohol (part of why drinking on an empty stomach hits faster), aspirin and some other small acidic drugs, and to a modest degree the smallest fats. But the bulk of absorption is deliberately deferred to the next organ.
Gastric emptying — the master pace-setter. The stomach releases its contents into the small intestine gradually, through a valve (the pylorus), at a controlled rate called the gastric emptying rate. This single variable controls how fast everything downstream happens — how quickly a drug takes effect, how fast blood sugar rises after a meal. What slows emptying: fat and protein in the meal, large volumes, high acidity, and certain hormones (e.g. GLP-1, the hormone that drugs like semaglutide mimic — slowed gastric emptying is a major reason they blunt appetite). What speeds it: liquids, simple carbohydrates, an empty-ish stomach. This is why "take on an empty stomach" means "absorb faster and more completely" (nothing slowing emptying, nothing to bind to), while "take with food" means slower, gentler, sometimes better-absorbed-if-fat-soluble.
Stop 4: The small intestine — where almost everything is absorbed
This is the main event. The overwhelming majority of nutrient and drug absorption happens in the small intestine, a long coiled tube (~6 metres) downstream of the stomach. It is built for absorption: its inner surface is folded, and covered in finger-like projections (villi), which are themselves covered in microscopic projections (microvilli, collectively called the brush border). This nesting of folds upon folds gives the small intestine an enormous absorptive surface area — roughly that of a tennis court.
The small intestine has three sections, in order: the duodenum (first, short), the jejunum (middle, the main absorptive workhorse), and the ileum (last, with some specialised jobs like absorbing vitamin B12 and recycling bile). Different things are absorbed preferentially in different sections, as we will see.
Before absorption can happen, two crucial secretions arrive in the duodenum:
- Bile, made by the liver and stored in the gallbladder, squirts in to handle fat (detailed below).
- Pancreatic enzymes and bicarbonate, from the pancreas. The bicarbonate neutralises the stomach acid (protecting the intestinal lining and giving the enzymes the near-neutral pH they need). The enzymes finish the chemical breakdown: pancreatic amylase (starch → sugars), proteases (proteins → amino acids and peptides), and lipase (fat → fatty acids).
Now let us follow each food type across the intestinal wall, because each one is absorbed by a different mechanism and routed onto a different highway.
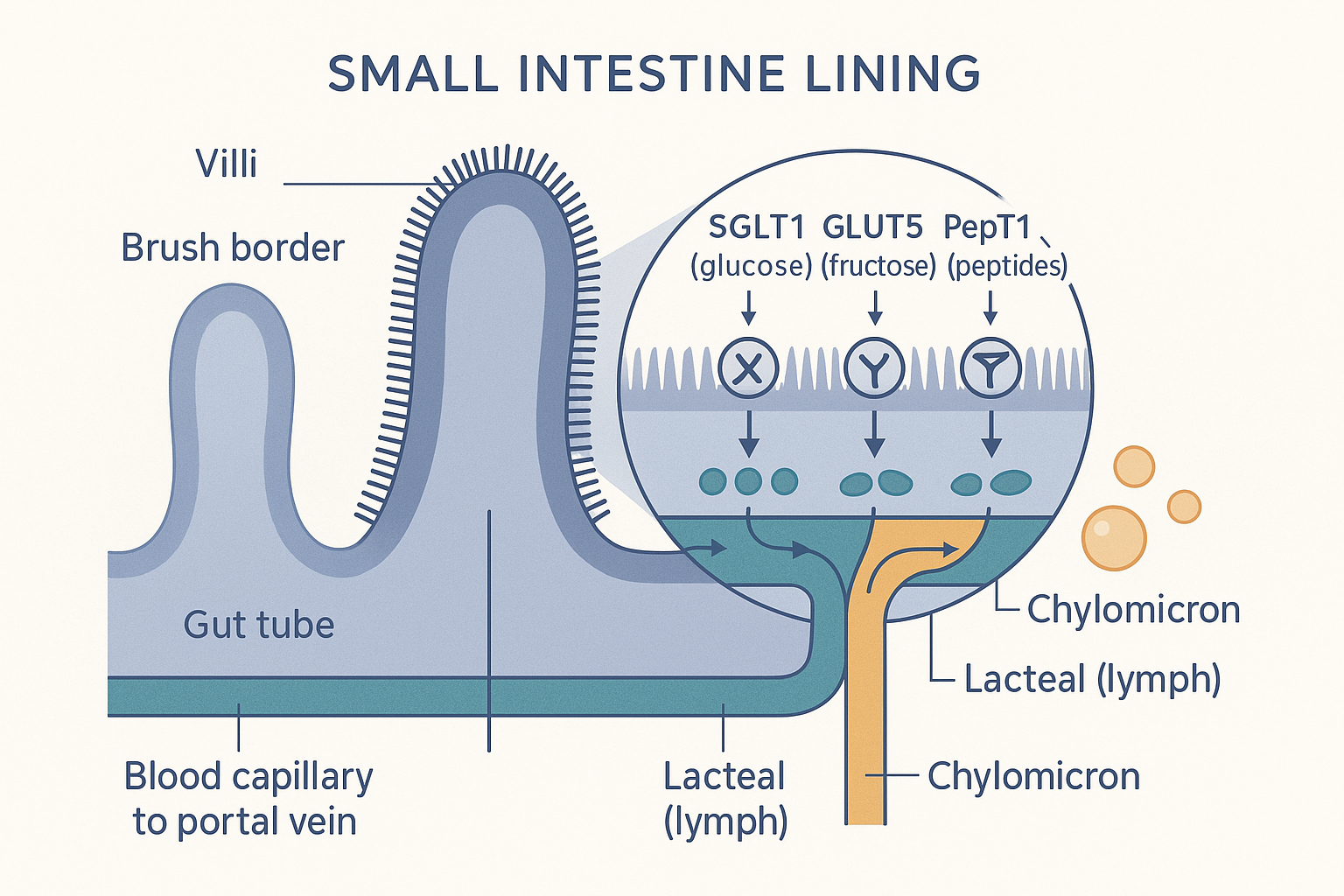 The absorbing surface: sugars and peptides cross via their transporters into the blood capillary (portal route), while fat packaged as chylomicrons enters the central lacteal (lymphatic route).
The absorbing surface: sugars and peptides cross via their transporters into the blood capillary (portal route), while fat packaged as chylomicrons enters the central lacteal (lymphatic route).
Carbohydrates → mostly the portal vein
Starches and sugars are broken all the way down to monosaccharides — single sugar units. There are three that matter: glucose, fructose, and galactose. They are absorbed across the brush border by specific transporter proteins (the same kind of doorway concept from the cellular energy page):
- Glucose and galactose ride in on a transporter called SGLT1, which co-transports them with sodium (an active, energy-using pump that can concentrate sugar even against a gradient).
- Fructose uses a different, passive doorway called GLUT5. This matters: fructose absorption is more limited and slower than glucose, and some people cannot absorb large fructose loads at all (the excess passes to the colon and ferments — a cause of bloating).
A common misconception worth correcting directly: people say "fructose goes straight to the liver" and imagine it being absorbed in the stomach or by some special shortcut. It is not. Fructose is absorbed in the upper small intestine like other sugars. The reason it "goes to the liver" is simply that, like all the sugars, it enters the portal vein — and the portal vein goes to the liver first. The difference is what the liver does with it: the liver is the primary site that metabolises fructose (whereas glucose largely passes through the liver and goes on to fuel the whole body). So fructose is not absorbed differently; it is processed differently once it arrives at the mandatory liver checkpoint. (The liver page covers why heavy fructose loads strain the liver.)
So: carbohydrates → portal vein → liver first. Glucose largely continues onward to fuel the body; fructose is mostly captured and dealt with by the liver.
Proteins → the portal vein
Proteins, already chopped by pepsin and pancreatic proteases, are broken down at the brush border into amino acids (single building blocks) and short peptides (two or three amino acids). These are absorbed by their own transporters — notably PepT1, which carries di- and tri-peptides. (This is the same transporter family that absorbs chelated minerals like magnesium glycinate, which is part of why those forms absorb well — they hitch a ride on the peptide doorway rather than competing at mineral doorways.)
Absorbed amino acids enter the portal vein → liver first. The liver takes first claim, using amino acids to build its own proteins, converting some to glucose or energy, and disposing of the nitrogen waste; the remainder passes on to the body. This is why dietary protein doesn't simply flood the bloodstream with amino acids — the liver buffers it.
This is also the destination of digested collagen and gelatin: they are proteins, broken down to amino acids and peptides like any other, and absorbed via the same route.
Fats → the lymphatic highway (the big exception)
Fat is where digestion gets genuinely different, and it explains several biohacking talking points.
Dietary fat arrives as triglycerides (a glycerol backbone with three fatty acid chains — the same storage form from the cellular energy page). Fat does not dissolve in the watery gut contents, so it would clump into useless globules. Bile solves this: bile acids act like a detergent, emulsifying the fat — breaking the globules into a fine suspension of tiny droplets, vastly increasing the surface area for the enzyme lipase to work on. Lipase then snips the fatty acids off the glycerol backbone. (Supplemental bile acids such as TUDCA relate to this step — bile is essential for fat and fat-soluble vitamin absorption, and poor bile flow impairs both.)
The freed fatty acids and other fat components, together with bile acids, assemble into even smaller packages called micelles, which ferry the fat right up to the brush border for absorption. So far so normal. But here is the twist that defines fat:
Once inside the intestinal cells, long-chain fatty acids are re-assembled back into triglycerides and packaged into large particles called chylomicrons. Chylomicrons are too big and too fatty to enter the blood capillaries directly. Instead they are dumped into the lymphatic system — the second highway. They travel through lymph vessels, eventually emptying into a large vein near the heart, entering the general circulation without passing through the liver first. The liver only processes the leftovers (chylomicron remnants) later.
flowchart TD
TG[Dietary triglycerides] -->|bile emulsifies| DROP[Tiny fat droplets]
DROP -->|lipase snips fatty acids| MIC[Micelles carry fat to brush border]
MIC --> ENT[Inside intestinal cell]
ENT -->|long-chain fat| CHYLO[Re-packaged into chylomicrons]
CHYLO ==>|too big for blood| LYMPH["LYMPHATIC highway<br/>→ bypasses liver"]
ENT -->|medium-chain fat / MCT| PORTAL["PORTAL vein<br/>→ liver first (fast)"]
LYMPH --> BODY[General circulation]
PORTAL --> LIVER[Liver]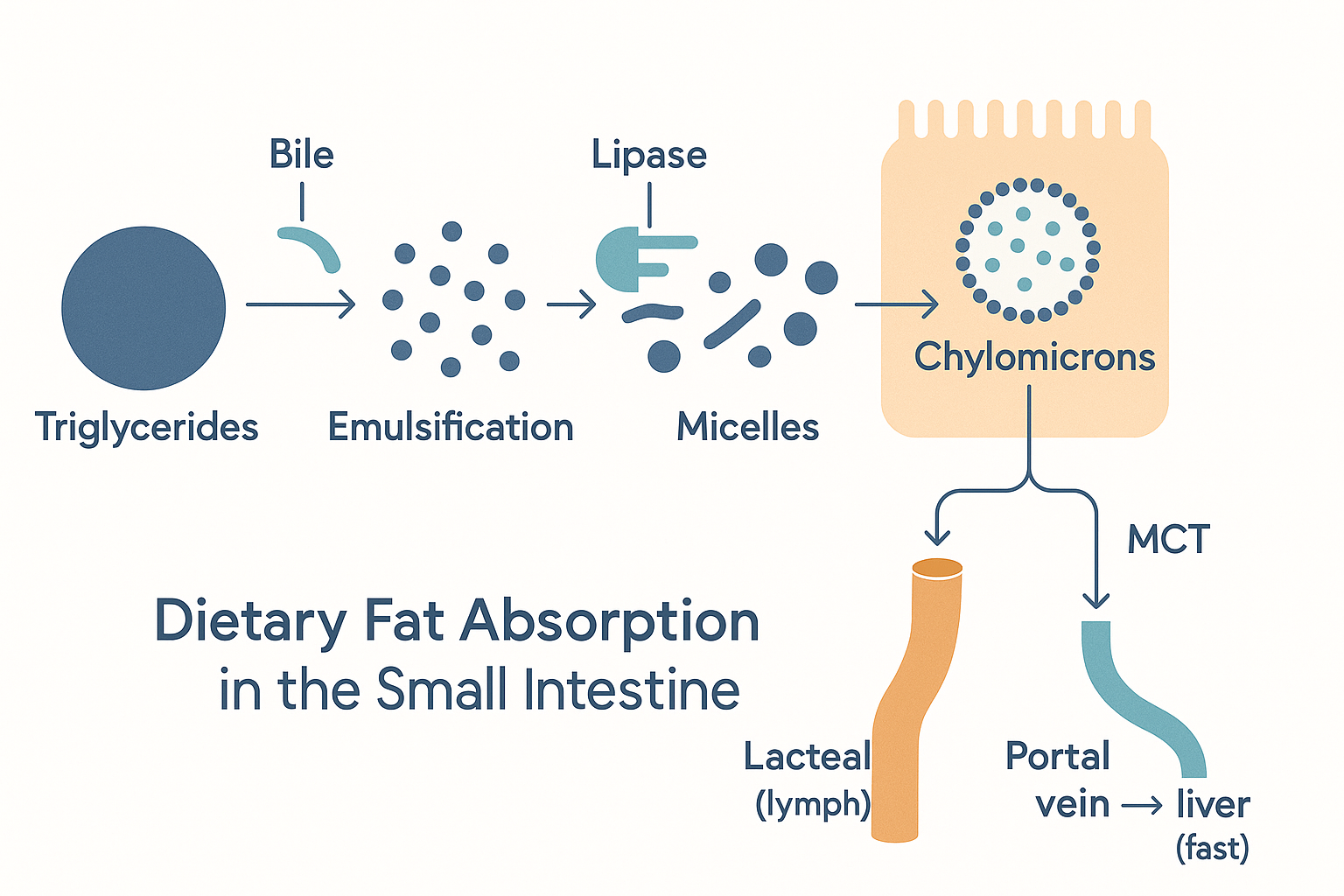 Fat's assembly line: bile and lipase break it down, micelles carry it in — then long-chain fat takes the slow lymphatic route while MCTs take the fast portal route to the liver.
Fat's assembly line: bile and lipase break it down, micelles carry it in — then long-chain fat takes the slow lymphatic route while MCTs take the fast portal route to the liver.
This is the mechanistic core of several claims:
- Why fat-soluble things have a slow, delayed onset — they take the long lymphatic detour rather than the direct portal route.
- Why coconut oil / MCTs are "special." Recall from the cellular energy page that medium-chain fatty acids (coconut oil / MCTs) behaved differently in the mitochondria. They behave differently here too: medium-chain fatty acids are small and water-soluble enough that they are not packaged into chylomicrons. Instead they are absorbed directly into the portal vein — the fast highway to the liver — where the liver can rapidly burn them or convert them to ketones. So MCTs take the carbohydrate-like fast route while normal long-chain fats take the slow lymphatic route. This is exactly why MCT oil is prized as a "fast" fat fuel.
Fat-soluble vitamins (A, D, E, K) → ride with the fat, on the lymphatic highway
The fat-soluble vitamins — vitamin A, D, E, and K (the "ADEK" group) — are absorbed by dissolving into the same micelles and chylomicrons as dietary fat, and they take the same lymphatic route. Two practical consequences follow directly:
- They must be taken with fat to be absorbed well. A fat-soluble vitamin swallowed with a fat-free meal is poorly absorbed — there is no fat to form the micelles that carry it in. This is why "take vitamin D with your largest/fattiest meal" is genuinely good advice, not folklore.
- They have a slower onset and are stored long-term, because they follow fat's slow, store-it-away logic rather than the fast portal route.
Water-soluble vitamins (B vitamins, C) → the portal vein, fast
The water-soluble vitamins — the B vitamins and vitamin C — dissolve in water, are absorbed by their own transporters in the small intestine, and enter the portal vein: the fast highway, liver first. They do not need fat, act faster, and are not stored in large reserves — excess is largely excreted (which is why water-soluble vitamins are generally less toxic in overdose than fat-soluble ones, and why they need more regular replenishment). One special case: vitamin B12 is absorbed only in the ileum (the last section of the small intestine) and only when bound to a stomach-made carrier protein called intrinsic factor — a multi-step dependency that makes B12 uniquely vulnerable to deficiency.
Stop 5: The portal vein and the liver's first-pass checkpoint
We have now sent almost everything water-soluble — sugars, amino acids, water-soluble vitamins, most drugs, alcohol — onto the portal vein. They all converge on the liver before reaching the body. This first-pass checkpoint is so important it deserves its own restatement:
- The liver captures and stores much of the incoming glucose as glycogen, buffering your blood sugar.
- The liver metabolises fructose and alcohol heavily here, which is why both place a disproportionate load on the liver.
- The liver takes first claim on amino acids, building proteins and disposing of nitrogen.
- The liver chemically transforms many drugs — sometimes inactivating them (so that a swallowed dose is largely destroyed before it works — the reason some drugs must be injected or taken sublingually), and sometimes activating them (some drugs are inert until the liver converts them — these are called prodrugs).
This is why the same molecule can have wildly different effects depending on the route it takes. Swallowed → portal vein → heavy first-pass. Sublingual, inhaled, injected, or (below) rectal → bypasses first-pass → far more reaches the body intact. The liver gets its own foundations page; here the key point is simply that the portal highway forces a mandatory liver checkpoint, and the lymphatic highway does not.
Stop 6: The large intestine (colon) — fibre, fermentation, and the bacterial economy
What reaches the large intestine (colon) is whatever the small intestine could not absorb: mainly fibre and other indigestible plant material, plus water and some residue. Two things happen here:
Water reabsorption. The colon reclaims water from the slurry, progressively solidifying the contents into stool. Too little water reabsorbed → diarrhoea; too much (slow transit) → constipation.
Bacterial fermentation. The colon houses trillions of bacteria (the gut microbiome, which gets its own foundations page). These bacteria ferment the fibre that your own enzymes could not break down. Fermentation of certain fibres produces short-chain fatty acids (SCFAs) — small molecules, principally butyrate, propionate, and acetate — which are genuinely useful:
- Butyrate is the preferred fuel for the cells lining the colon itself (colonocytes) — they run largely on it. It also helps maintain the gut barrier and has anti-inflammatory effects.
- Propionate is absorbed into the portal vein and travels to the liver, where it influences glucose handling.
- Acetate enters the general circulation and can be used as fuel by other tissues.
This is why fermentable fibre (and supplements like resistant starch) is described as "feeding the gut" — you are literally feeding the bacteria that produce butyrate for your colon. (Which fibres feed beneficial versus harmful bacteria is a more nuanced question taken up on the gut microbiome page — not all fibre is equal.)
Stop 7: The rectal route — the other deliberate liver bypass
A useful coda. The lower colon and rectum can absorb some substances directly across their wall — and the lower rectal veins drain partly into the general circulation rather than the portal vein. This means a substance delivered rectally (a suppository, or an enema) can partially bypass first-pass liver metabolism, much like the sublingual route does at the other end. This is why some medications are given rectally (when first-pass would destroy them, or when a patient cannot swallow), and it is the mechanistic basis for the various enema-based protocols in the biohacking world. It is the colon's version of the sublingual shortcut.
Putting it all together: a molecule's-eye view
The whole journey, compressed:
- Mouth: chew (surface area), salivary amylase starts on starch; sublingual route can absorb small fat-soluble potent molecules directly into blood, bypassing the liver.
- Stomach: acid + pepsin denature and start breaking protein; gastric emptying rate sets the pace for everything downstream; little is absorbed except alcohol and a few small drugs.
- Small intestine (the main event): bile emulsifies fat, pancreatic enzymes finish breakdown, and the tennis-court surface absorbs nearly everything —
- carbohydrates (SGLT1 / GLUT5) → portal vein → liver first
- amino acids & peptides (PepT1) → portal vein → liver first
- long-chain fats → chylomicrons → lymphatic highway → bypass liver
- fat-soluble vitamins A/D/E/K → ride with fat → lymphatic, need dietary fat, slow onset
- water-soluble vitamins (B, C) → portal vein, fast, not stored
- MCTs → behave like sugar → portal vein, fast
- Liver first-pass: everything on the portal highway is inspected — glucose stored, fructose and alcohol metabolised, amino acids claimed, drugs activated or destroyed.
- Colon: water reclaimed; bacteria ferment fibre into SCFAs (butyrate fuels the colon); rectal route can bypass the liver.
Once past all this, the molecules are finally in the general circulation and arrive at the cells — where, for fuel molecules, the cellular energy story begins.
The single sentence to remember: water-soluble things take the portal highway and meet the liver first; fat takes the lymphatic highway and skips it — and almost every practical rule about how to take a supplement follows from which highway it rides.
flowchart LR
CARB["Carbohydrates<br/>(glucose, fructose)"] --> PORTAL
PROT["Protein<br/>(amino acids, peptides)"] --> PORTAL
WSV["Water-soluble vitamins<br/>(B, C)"] --> PORTAL
MCT["MCTs / coconut oil"] --> PORTAL
ALC[Alcohol, most drugs] --> PORTAL
PORTAL["PORTAL VEIN<br/>→ liver first (first-pass)"]
LCF["Long-chain fat"] --> LYMPH
FSV["Fat-soluble vitamins<br/>(A, D, E, K)"] --> LYMPH
LYMPH["LYMPHATIC<br/>→ skips liver"]
SUB["Sublingual / rectal"] --> BYPASS["Straight to blood<br/>→ skips liver"]Related Compounds & Deep Dives
Stomach acid & protein digestion
- Betaine HCl — lowers stomach pH to support pepsin activation and protein breakdown when stomach acid is low.
- Apple cider vinegar — acidifies the stomach for the same reason; a milder, dietary version.
Fat & bile
- TUDCA — a bile acid; bile is essential for emulsifying fat and absorbing fat-soluble vitamins, so bile flow gates this entire route.
- Coconut oil / MCTs — medium-chain fats that skip the chylomicron/lymphatic route and take the fast portal highway to the liver.
Vitamins, by highway
- Vitamin D, E, K, ADEK group — fat-soluble; must be taken with dietary fat, travel the lymphatic route, slow onset, stored long-term.
- B vitamins, Vitamin C — water-soluble; portal route, fast, not stored, need regular replenishment.
Colon, fibre & SCFAs
- Butyrate — the short-chain fatty acid that is the colon lining's preferred fuel; the end-product of fibre fermentation.
- Resistant starch — fermentable fibre that feeds butyrate-producing colon bacteria.
Gut barrier & lining
- L-glutamine, Zinc-L-carnosine, BPC-157, Larazotide — support the integrity of the intestinal wall across which all this absorption happens.
Specialised digestion
- DAO (diamine oxidase) — the gut enzyme that breaks down dietary histamine.
- Aspirin — one of the few drugs absorbed partly in the acidic stomach.
Related foundations
- Cellular Energy — what happens to glucose and fatty acids after absorption, once they reach the cell.