Hepatic Load: Why Drugs and Supplements Burden the Liver
Almost everything you swallow is routed through the liver before it reaches the rest of you — and the liver has to chemically dismantle each one. "Hepatic load" is the total processing demand that places on the organ. This page explains what that demand actually is, why stacking multiple compounds is more than the sum of its parts, how a molecule physically damages liver cells, and what "being careful" concretely means — using a deworming protocol as the worked example.
Read alongside
This page builds directly on the Liver foundations page — especially Job 7, the three-phase detox pipeline — and on the Digestion page, which explains why the liver sees everything first (the portal vein). It is the pharmacological companion to the Deworming Protocol and Gut Reset Protocol, where multiple compounds are run at once.
Why this page exists
People in protocol-heavy corners of biohacking stack a lot of compounds at once — a deworming course, gut-reset antimicrobials, a cognitive stack, a sleep stack — and the standing warning, repeated on nearly every page of this site, is "these require medical supervision." That warning usually lands as vague anxiety rather than understanding. The single most important reason behind it is hepatic load, and once you see the mechanism it stops being mystical.
The puzzle most people start with is: why would a supplement "burden" the liver at all? It's just a pill. The answer is that your liver does not know or care whether a molecule is a prescription drug, a veterinary dewormer, a herbal extract, or a vitamin. To the liver they are all xenobiotics — foreign chemicals it must identify, chemically transform, and dispatch for excretion. Every one of them queues for the same finite processing machinery. Load is simply how much work is in that queue, and how dangerous the work is.
First, the plumbing: why the liver is first in line
From the digestion page: almost everything water-soluble you absorb from the gut — sugars, amino acids, alcohol, and most oral drugs and supplements — does not go straight into general circulation. It is collected into the hepatic portal vein and delivered to the liver first, before it reaches the heart, brain, or anywhere else.
This has a name: first-pass metabolism. Before an oral compound ever reaches its target, the liver gets first crack at it. For many drugs the liver destroys a large fraction on this first pass (which is why oral doses are often much larger than injected ones). The flip side is the point of this page: the liver absorbs the chemical workload of nearly everything you take by mouth, up front, in concentrated form. Whatever you swallow, the liver pays first.
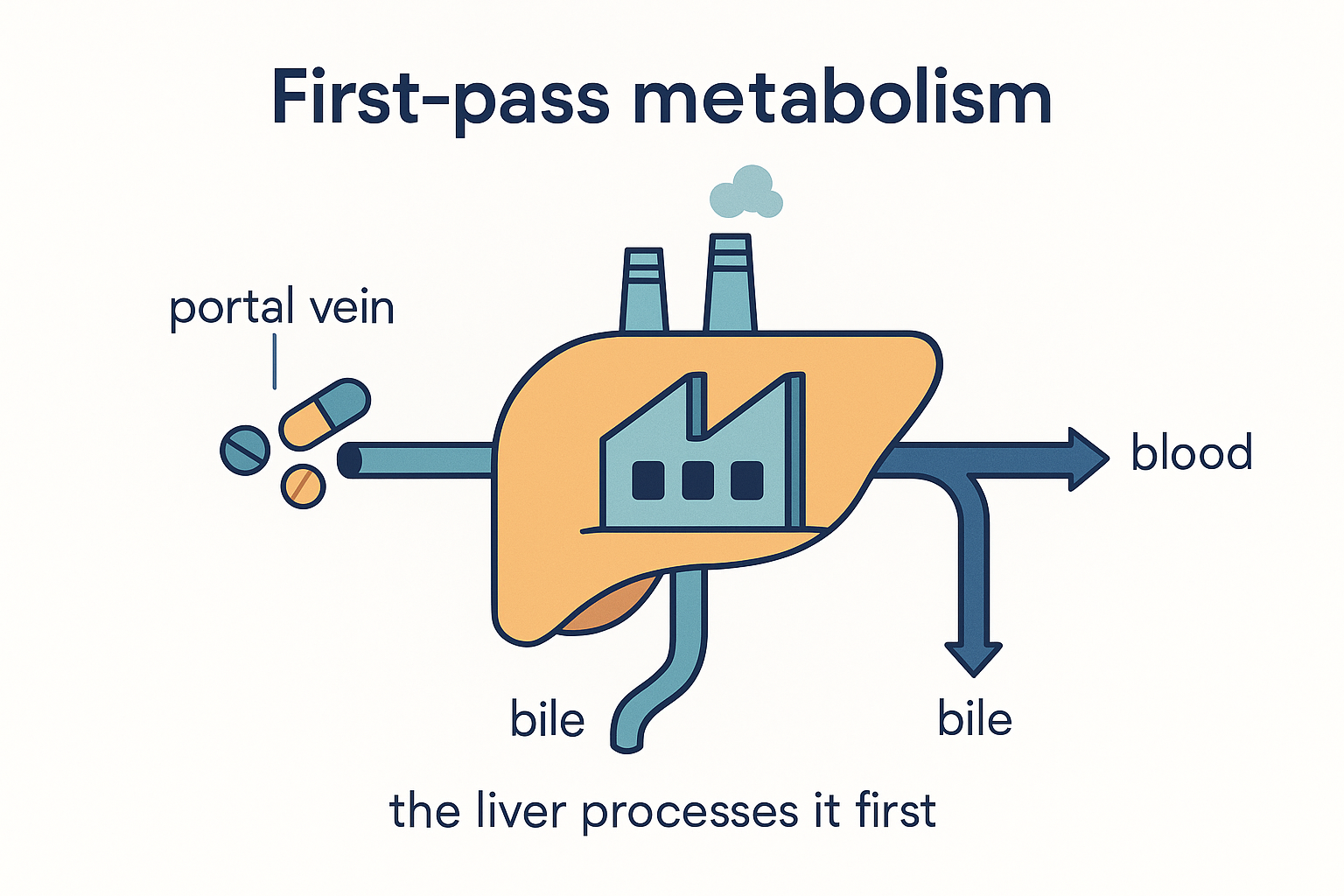 Everything water-soluble you swallow is delivered to the liver first, in concentrated form — it pays the chemical bill before the rest of you ever sees the molecule.
Everything water-soluble you swallow is delivered to the liver first, in concentrated form — it pays the chemical bill before the rest of you ever sees the molecule.
What the liver actually does to a foreign molecule
The liver page's Job 7 covers this in full; here is the compressed version, because the load concept lives entirely inside it.
Most xenobiotics are fat-soluble — which is how they got absorbed and how they cross into cells. The problem is that fat-soluble molecules cannot be excreted easily; the kidneys can only flush water-soluble things. So the liver runs a two-step conversion to make them water-soluble and safe:
- Phase I (transformation) — the cytochrome P450 (CYP) enzymes. A large family of liver enzymes chemically modify the molecule, usually by oxidation. The catch, and it is the crucial one: Phase I frequently makes the molecule more reactive and more toxic, not less. It produces an unstable intermediate that is supposed to be neutralised immediately by the next step.
- Phase II (conjugation) — making it safe. The liver bolts a water-loving handle (glucuronic acid, sulphate, or glutathione) onto the reactive intermediate, neutralising it and making it excretable.
- Phase III (transport out). Pumps move the finished, safe conjugate into bile (out via the gut) or blood (out via the kidneys).
flowchart LR
DRUG["Drug / supplement<br/>(fat-soluble)"] -->|"Phase I<br/>CYP450"| INT["Reactive intermediate<br/>(often MORE toxic)"]
INT -->|"Phase II<br/>+ glutathione / glucuronide / sulphate"| SAFE["Safe, water-soluble"]
SAFE -->|"Phase III"| OUT["Bile or urine"]
INT -. "if Phase II can't keep up" .-> DMG["Reactive intermediate<br/>attacks the cell"]The single engineering insight to carry forward: detox is a two-step pipeline where the middle product is the most dangerous thing in it. Phase I and Phase II must stay balanced. Load becomes damage precisely when the dangerous middle stage backs up.
What "load" really is: three ways the queue overflows
"Hepatic load" is not one thing. It is the sum of three distinct pressures on that pipeline.
1. Volume — the raw amount of work
The most obvious: more compound, more molecules to process. This scales with dose and duration. A single 100mg dose is trivial; 500mg/day of a benzimidazole for four weeks is a sustained, high-volume job. This is why the cancer-tier dosing in the deworming page (50–100 mg/kg mebendazole) sits in a completely different risk category from a one-off pinworm dose — same drug, vastly different load.
2. The traffic jam — competition for shared enzymes
Here is the part that makes stacking more dangerous than any single item suggests. The CYP enzyme family is large, but a handful of enzymes do most of the work — and one enzyme, CYP3A4, metabolises an estimated half of all drugs. When several compounds all depend on the same enzyme, they compete for it.
Think of CYP3A4 as a single checkout lane that much of your traffic funnels through:
- If two compounds both need CYP3A4, each slows the other's clearance. Blood levels of both rise higher and last longer than either would alone.
- Some compounds inhibit the enzyme outright (the textbook example is grapefruit, which knocks out gut CYP3A4 — drugs cleared by it then build up to dangerous levels). Others induce it (ramp it up), which can clear a co-administered drug too fast to work.
flowchart TD
A["Compound A"] --> CYP{"CYP3A4<br/>(one shared lane)"}
B["Compound B"] --> CYP
C["Compound C"] --> CYP
CYP -->|"clearance slows<br/>for all three"| BUILD["Levels rise & linger<br/>→ higher peak load,<br/>more reactive intermediate"]
GF["Grapefruit / inhibitors"] -. "block the lane" .-> CYPThe consequence: a stack's load is not additive — it is interactive. Three compounds that each clear cleanly in isolation can, together, jam the lane, raise each other's peak concentrations, and generate more reactive intermediate than the Phase II side was provisioned for.
3. The glutathione tax — depleting the safety supply
Phase II's most important neutraliser, glutathione, is a consumable. Every reactive intermediate it quenches uses up a glutathione molecule, and the liver has a finite pool it must continually regenerate. A heavy, sustained Phase I workload draws down glutathione faster than it is replenished. When the pool runs low, reactive intermediates start escaping un-neutralised — and that is when load tips into injury.
This is not theoretical. It is the exact mechanism of paracetamol (acetaminophen) poisoning: a normally-minor toxic intermediate (NAPQI) is safely mopped up by glutathione at normal doses, but an overdose — or a normal dose on an already-depleted pool (fasting, alcohol, malnutrition) — exhausts the glutathione, and the freed intermediate destroys liver cells. The hospital antidote is NAC, which works for one reason only: it rebuilds glutathione. Hold onto this — it is the template for everything in the "support" section below.
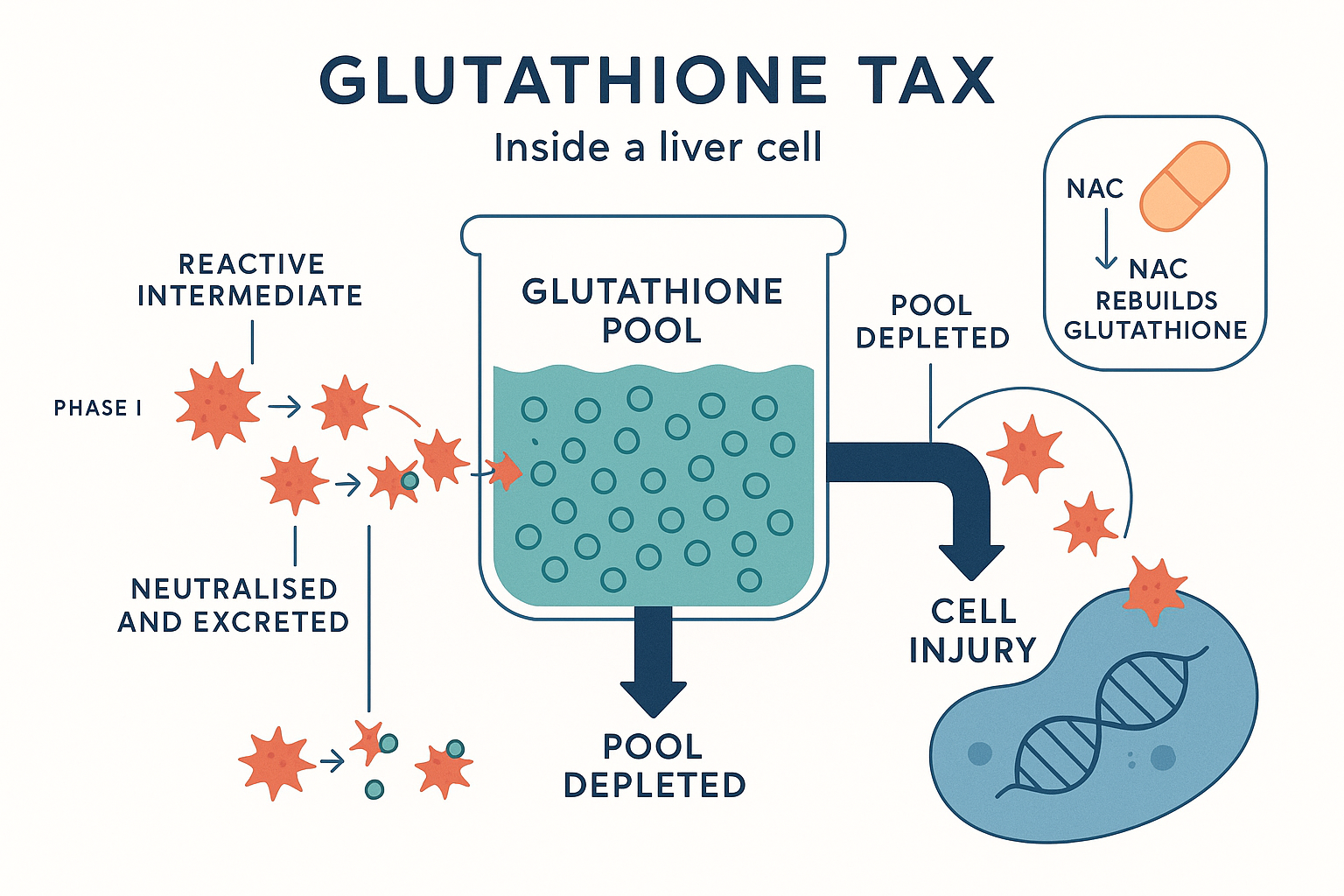 Glutathione is a consumable: a heavy Phase I workload drains the finite pool faster than it refills, and injury begins the moment reactive intermediates start escaping un-neutralised — the exact mechanism of paracetamol poisoning, and why NAC (which rebuilds glutathione) is the antidote.
Glutathione is a consumable: a heavy Phase I workload drains the finite pool faster than it refills, and injury begins the moment reactive intermediates start escaping un-neutralised — the exact mechanism of paracetamol poisoning, and why NAC (which rebuilds glutathione) is the antidote.
How a molecule actually damages the liver
"Hepatotoxicity" (liver injury from a chemical) is a real, mechanistic event, not a vibe. The main routes:
- Reactive intermediate attack. As above: a Phase I product escapes Phase II and covalently binds to and damages cellular proteins, membranes, and DNA. The dominant mechanism for dose-dependent injury.
- Mitochondrial injury. Some compounds poison the hepatocyte's mitochondria directly, starving the cell of energy. (Recall from cellular energy that the liver is metabolically the busiest organ — it is acutely sensitive to mitochondrial damage.)
- Cholestasis. Others jam the bile export machinery (Phase III), so bile and its components back up inside the liver and become toxic. This shows up as itching and jaundice rather than pure enzyme leakage.
- Immune-mediated injury. Occasionally a drug-protein adduct is flagged as foreign and the immune system attacks the liver — idiosyncratic, not dose-dependent, and unpredictable.
How do you see this happening? When hepatocytes are injured, they leak their internal enzymes — ALT and AST (the "transaminases") — into the blood. A liver function test (LFT) measuring raised ALT/AST is the smoke alarm: it tells you cells are being damaged, usually well before you feel anything. This is the entire reason for blood monitoring during heavy protocols — symptoms (fatigue, nausea, right-upper-abdomen ache, dark urine, yellowing eyes) often appear late, after meaningful damage. The bloods catch it early.
The worked example: a triple-drug deworming stack
Now apply all of this to the protocol this page accompanies. A common stack runs ivermectin + a benzimidazole, daily, in pulses, for weeks. Where does the load come from?
- Benzimidazoles — fenbendazole and mebendazole (and their cousin albendazole) are cleared by the liver and are the heavy items here. At deworming doses they are usually well tolerated, but at high doses or prolonged use they are a recognised cause of raised transaminases and, occasionally, real liver injury — which is exactly why the high-dose "Joe Tippens"-style and cancer-tier regimens carry the most hepatic risk. Sustained dosing over weeks is a volume load.
- Ivermectin is metabolised primarily by CYP3A4 — the shared lane. At antiparasitic doses hepatotoxicity is uncommon (its dose-limiting risk is neurological at very high doses), but it occupies CYP3A4, so it contributes to the traffic jam rather than being a big standalone load.
The dual-benzimidazole trap
Fenbendazole and mebendazole share a virtually identical mechanism — they are essentially the veterinary and human versions of the same drug. Taking both together doubles the hepatic volume load without killing any more parasites. As the deworming page states plainly, most protocols pick one. Running both is the clearest avoidable way to inflate hepatic load for zero benefit. Choose mebendazole (regulated, human-grade) or fenbendazole — not both.
Stack the three pressures and the picture is clear: a sustained-volume benzimidazole load, running through a CYP3A4 lane also occupied by ivermectin, drawing on a glutathione pool over a multi-week course. None of it is necessarily dangerous at sensible single-drug doses — but it is precisely the situation where dose, duration, and what else you add determine whether the pipeline stays balanced.
Not everything loads the liver equally
This is the calibration that prevents the whole idea from collapsing into "everything is bad for your liver." It is not true, and the differences are large and mechanistic.
- Heavy hepatic load: orally-dosed, fat-soluble small-molecule drugs that depend on CYP metabolism and/or generate reactive intermediates — the benzimidazoles here, many pharmaceuticals, high-dose lipophilic compounds, and alcohol (which additionally drains the liver's NAD⁺; see liver Job 9).
- Light hepatic load: much of a typical cognitive/sleep stack actually passes the liver lightly —
- Peptides like pinealon and epithalon are short amino-acid chains broken down by ordinary peptidases, not the CYP system — minimal CYP load.
- Minerals like magnesium (incl. L-threonate) are handled as ions, not detoxified through Phase I/II.
- Water-soluble vitamins like the B1 forms (benfotiamine, TTFD) are low-burden and largely renally cleared.
⚖️ Calibration. "Supports the liver" and "burdens the liver" are both thrown around far too loosely. The honest version: load is dominated by fat-soluble drugs that run the CYP gauntlet and spend glutathione, scaled by dose and duration and amplified by enzyme competition. A peptide, a mineral, and a B-vitamin are not meaningfully in that category. In the worked example, the load is almost entirely the antiparasitics — the cognitive stack riding alongside is comparatively light. That is why it matters which items you're careful about: misplaced worry about the peptides distracts from the real variable, which is the dose, duration, and doubling-up of the dewormers.
What "being careful" concretely means
This is the actionable payoff. "Be careful with your liver" decomposes into specific, mechanism-derived moves:
Reduce the load itself
- Don't double up same-mechanism drugs (the benzimidazole trap above). One dewormer, not two.
- Respect dose and duration. Lower and shorter is lower load. Pulsing (e.g. three days on, four off) gives the liver recovery windows and lowers cumulative volume versus continuous dosing — one reason pulsed deworming schedules are sensible beyond just catching egg-hatch cycles.
- Avoid stacking unnecessary CYP3A4 traffic during the course — and note the classics that jam the lane: grapefruit juice, and alcohol (which both competes and depletes NAD⁺ and glutathione). Removing alcohol during a heavy protocol is one of the highest-leverage moves.
- Be cautious with paracetamol during the course — it spends the same glutathione you're already drawing down.
Support the pipeline (stock the raw materials Phase II runs on)
The liver page makes the key point: "liver support" is not a detox tea — it is supplying the consumables the conjugation steps depend on. The ones with a real mechanistic basis:
- NAC and glutathione — replenish the master Phase II neutraliser that a heavy Phase I load depletes. This is the single most mechanistically-justified support.
- Glycine and taurine — amino acids used in Phase II conjugation and in bile-acid formation (and conveniently already in the gut-reset stack).
- Selenium — cofactor for glutathione-peroxidase, part of the antioxidant defence.
- TUDCA — supports bile flow, the Phase III export route, helping clear the finished conjugates (and guarding against the cholestasis route of injury).
- Curcumin — studied for protecting hepatocytes from oxidative/inflammatory stress.
Watch the smoke alarm
- For any sustained, high-dose, or multi-drug course, baseline and periodic LFTs (ALT/AST) are how you catch injury early — before symptoms. This is the concrete thing "medical supervision" buys you, and the reason it is not optional advice on the protocol pages.
- Know the late warning signs that mean stop and seek help: persistent nausea, right-upper-abdominal pain, unusual fatigue, dark urine, pale stools, yellowing of skin or eyes.
flowchart TD
LOAD["HEPATIC LOAD"] --> V["Volume<br/>(dose × duration)"]
LOAD --> J["Enzyme competition<br/>(shared CYP3A4 lane)"]
LOAD --> G["Glutathione drawdown"]
V & J & G --> BAL{"Phase I / Phase II<br/>balance holds?"}
BAL -->|yes| OK["Cleared safely"]
BAL -->|no| INJ["Reactive intermediates escape<br/>→ ALT/AST rise → injury"]
SUP["Lower dose · pulse · drop alcohol/grapefruit ·<br/>stock glutathione (NAC) · bile flow (TUDCA) ·<br/>monitor LFTs"] -. shifts balance toward .-> OKPutting it all together
- First-pass position: nearly everything you swallow hits the liver first and in concentrated form — the liver pays the chemical bill up front.
- The pipeline: Phase I makes molecules more reactive, Phase II neutralises them, Phase III exports them. Damage happens when the dangerous middle stage backs up.
- Load = volume + competition + glutathione tax. Dose and duration set the volume; shared CYP enzymes (especially CYP3A4) make stacks interactive, not additive; sustained Phase I work depletes the finite glutathione that keeps the pipeline safe.
- Injury is reactive-intermediate attack, mitochondrial poisoning, cholestasis, or immune reaction — and it shows up as raised ALT/AST before you feel it.
- Not everything loads equally: fat-soluble CYP-metabolised drugs (and alcohol) are the heavy items; peptides, minerals, and water-soluble vitamins are light. In a deworming stack the load is overwhelmingly the antiparasitics, and doubling up two same-mechanism benzimidazoles is pure avoidable load.
- Being careful = don't double up, respect dose/duration, pulse, drop alcohol/grapefruit/paracetamol, stock the Phase II consumables (glutathione via NAC, glycine, taurine, selenium; bile flow via TUDCA), and monitor LFTs — which is exactly what supervision provides.
The unifying idea mirrors the liver page's own conclusion: the liver is a finite transformer with a finite safety supply. Hepatic load is just how hard you are running it and how fast you are spending its safety margin. You manage it by sending less dangerous work through, and by keeping the safety supply stocked.
Educational only. Not medical advice. Multi-compound protocols involving prescription or off-label drugs genuinely warrant baseline and follow-up bloods and clinical oversight — this page is an explanation of why, not a substitute for it.
Related Compounds & Deep Dives
The machinery
- Liver foundations page — the full anatomy of the detox pipeline and the liver's other jobs.
- Digestion — the portal vein and why the liver is first in line.
- Cellular Energy — the mitochondria and NAD⁺ that alcohol and some toxins drain.
The worked example
- Deworming Protocol and Gut Reset Protocol — the multi-compound courses this load analysis applies to.
- Fenbendazole, Mebendazole, Ivermectin — the antiparasitics and their hepatic handling.
Supporting the pipeline