Cerebrolysin — Deep Dive
A standardised soup of pig-brain peptides, injected to make a damaged human brain repair itself — and the widest gap in this database between community conviction and Western trial data.
Category: Neuropeptide preparation / Neurotrophic / Neurorestorative Manufacturer: EVER Neuro Pharma (Austria) Developed by: Gerhart Harrer (clinical neurologist/psychiatrist, mid-20th century) Composition: Standardised enzymatic hydrolysate of purified porcine brain proteins — low-molecular-weight neuropeptides (<10 kDa) + free amino acids Route: Intramuscular (IM) or intravenous (IV) — degrades if swallowed Status: Approved drug in 50+ countries (Russia, China, much of Eastern Europe, parts of Asia/Latin America). Not FDA-approved. Not EMA-approved.
The thing you have to accept first: this is not a molecule
Almost every other compound in this database is a defined chemical. BPC-157 is fifteen amino acids in a known sequence. Modafinil is a single structure with a CAS number. You can draw them.
Cerebrolysin you cannot draw. It is a mixture — and not a vague one, a standardised one, which is the whole pharmaceutical trick. The starting material is purified pig brain. That brain tissue is delipidated (fat removed) and its proteins are then chopped up by controlled enzymatic proteolysis — the same kind of process that turns milk protein into a whey hydrolysate. What comes out the other end is a defined-by-spec broth: roughly 75% free L-amino acids (17 of them) and roughly 25% low-molecular-weight peptides, all under ~10 kDa, at a fixed peptide concentration (215.2 mg/mL of peptide concentrate in the standard solution). Each batch is held to a specification, not a single formula (ScienceDirect overview; superpower.com guide).
Morph (@doctormorphh) puts the provocation bluntly:
"Inject yourself with pig brains to become smarter? … Cerebrolysin is a neuropeptide that is obtained by enzymatic proteolysis from pig brains."
That is genuinely what it is. The interesting question is why a brain hydrolysate would do anything coherent — and the answer is the entire reason this page exists.
flowchart LR
PIG["Purified porcine<br/>brain tissue"] --> DELIP["Delipidation<br/>(remove fat)"]
DELIP --> PROT["Controlled enzymatic<br/>proteolysis"]
PROT --> FILTER["Filtration +<br/>standardisation to spec"]
FILTER --> MIX["Defined mixture:<br/>~75% free amino acids<br/>~25% peptides (<10 kDa)"]
MIX --> AMP["Ampoule<br/>(aqueous, IM/IV)"]Brain → broth → ampoule. The peptides are not synthesised; they are the surviving fragments of real neural proteins, cut to a size that can act on cells but is too small to be a whole protein.
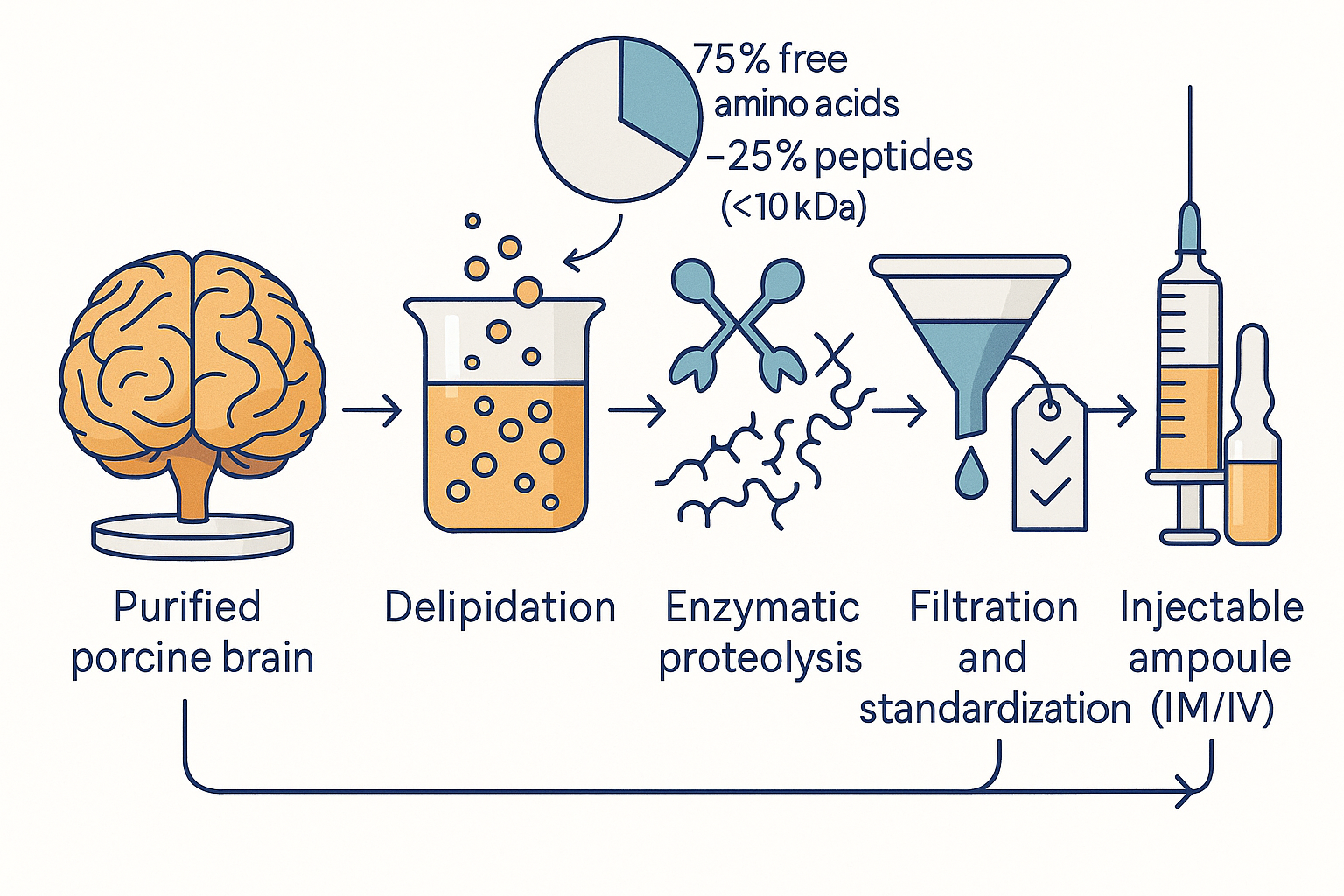 From pig brain to standardised ampoule: the peptides are surviving fragments of real neural proteins, cut small enough to signal but too small to be whole proteins — and the per-batch specification is what makes a "soup" a pharmaceutical.
From pig brain to standardised ampoule: the peptides are surviving fragments of real neural proteins, cut small enough to signal but too small to be whole proteins — and the per-batch specification is what makes a "soup" a pharmaceutical.
First principles: why you can't just take BDNF
To understand what Cerebrolysin is trying to be, start with what the brain uses to repair and remodel itself: neurotrophic factors.
These are the brain's own growth and survival proteins — BDNF (brain-derived neurotrophic factor), NGF (nerve growth factor), GDNF (glial-derived neurotrophic factor), CNTF (ciliary neurotrophic factor), IGF-1 (insulin-like growth factor 1). They do the heavy lifting of neuroplasticity: keeping neurons alive, growing new synapses, driving the birth of new neurons (neurogenesis) in the hippocampus, and protecting tissue from the cell-death cascades that follow a stroke or a concussion. (The Semax & Selank deep dive covers the BDNF/TrkB axis in detail; this page assumes that foundation.)
So the obvious biohacker move is: just take BDNF. You can't. BDNF is a ~27 kDa protein. Two hard walls stop it:
- It doesn't cross the blood-brain barrier. Large proteins injected into the bloodstream simply don't reach brain parenchyma in meaningful amounts.
- It's unstable and short-lived. Recombinant BDNF has a plasma half-life measured in minutes and is degraded by peptidases.
This is the same wall every neurotrophic-factor drug programme has hit. Trials of recombinant BDNF, CNTF, NGF and GDNF for ALS, Alzheimer's and Parkinson's have repeatedly failed — not because the biology was wrong, but because you cannot get an intact trophic protein to the right neurons at the right concentration.
Cerebrolysin is a sideways answer to that wall. Instead of delivering a whole, fragile, barrier-excluded protein, it delivers small fragments — peptides under 10 kDa, in the size range that can plausibly cross a compromised blood-brain barrier (and the barrier is compromised exactly where it matters: stroke, TBI, neuroinflammation). Some of those fragments are thought to act as neurotrophic-factor mimetics — short enough to be stable, small enough to move, shaped enough to engage the same Trk-receptor signalling that BDNF and NGF use (realpeptides.co mechanism).
That is the conceptual bridge: a brain hydrolysate is an attempt to deliver the signal of neurotrophic factors without delivering the molecules of neurotrophic factors.
The mechanism: whole-cascade, not single-target
Here is the thesis that the community — and Morph in particular — keeps returning to, and it is the single most important idea on this page.
"Its special because its not selective of which neurotrophic factors it increases compared to other nootropics. Cognitive enhancement cant be dumbed down to 'increase BDNF' or 'muh SHH' because pathways are interdependent and need to be active in synchrony to work effectively. Which is why nootropics that work very selective work very well for people deficient in that specific aspect but lacks efficacy in people who arent deficient in that specific signal… Compared to other nootropics, cerebrolysin potentiates entire signaling cascades; providing a balanced and synchronized enhancement."
Strip the enthusiasm and there's a real pharmacological argument underneath. A single-target nootropic — say, a pure BDNF-inducer — only helps if BDNF is your rate-limiting step. If your bottleneck is elsewhere (vascular supply, inflammation, IGF-1 signalling), the single-target drug does little. Cerebrolysin's pitch is that it nudges the whole interdependent network at once, so it doesn't need to guess which signal is limiting.
Mechanistically, two things are claimed to happen, and they're worth separating:
1. Direct mimicry. Some peptide fragments act like trophic factors — engaging Trk receptors and firing the canonical survival/plasticity pathways: PI3K → Akt (the anti-apoptotic survival arm) and MAPK/ERK → CREB (the gene-transcription arm that builds synapses and underwrites long-term potentiation).
2. Endogenous amplification. Cerebrolysin also appears to stimulate the brain's own cells — neurons, glia, endothelium — to produce more BDNF, VEGF and IGF-1, while turning down the pro-inflammatory cytokine TNF-α (realpeptides.co; PeptideInsight). So it is partly a mimic and partly a trigger — it doesn't just push the signal, it asks the tissue to make more of its own.
The downstream effects Morph lists map cleanly onto established neurobiology:
flowchart TD
CB((Cerebrolysin)) --> TROPH["Neurotrophic signalling<br/>BDNF · NGF · GDNF · CNTF · IGF-1"]
CB --> SHH["Sonic Hedgehog (SHH)<br/>pathway"]
CB --> VASC["VEGF · Ang1<br/>(vascular)"]
TROPH --> SURV["PI3K/Akt<br/>survival arm"]
TROPH --> PLAST["MAPK/ERK → CREB<br/>plasticity arm"]
SURV --> APO["Anti-apoptosis:<br/>↑Bcl-2 ↓Bax<br/>calpain inhibition"]
PLAST --> SYN["New synapses · LTP ·<br/>hippocampal neurogenesis"]
SHH --> NEUROG["Neurogenesis<br/>(SVZ + dentate gyrus)"]
VASC --> ANGIO["Angiogenesis<br/>(new vessels into damaged tissue)"]
CB --> INFLAM["↓TNF-α · microglial<br/>modulation"]
CB --> EXCITO["↓Glutamate<br/>excitotoxicity"]
APO --> REPAIR["Neuroprotection +<br/>neurorestoration"]
SYN --> REPAIR
NEUROG --> REPAIR
ANGIO --> REPAIR
INFLAM --> REPAIR
EXCITO --> REPAIRThe "synchronised whole-cascade" picture: Cerebrolysin is claimed to touch the trophic, vascular, anti-apoptotic, neurogenic and anti-inflammatory arms simultaneously — which is exactly why its mechanism is easy to describe and its clinical effect is hard to pin down.
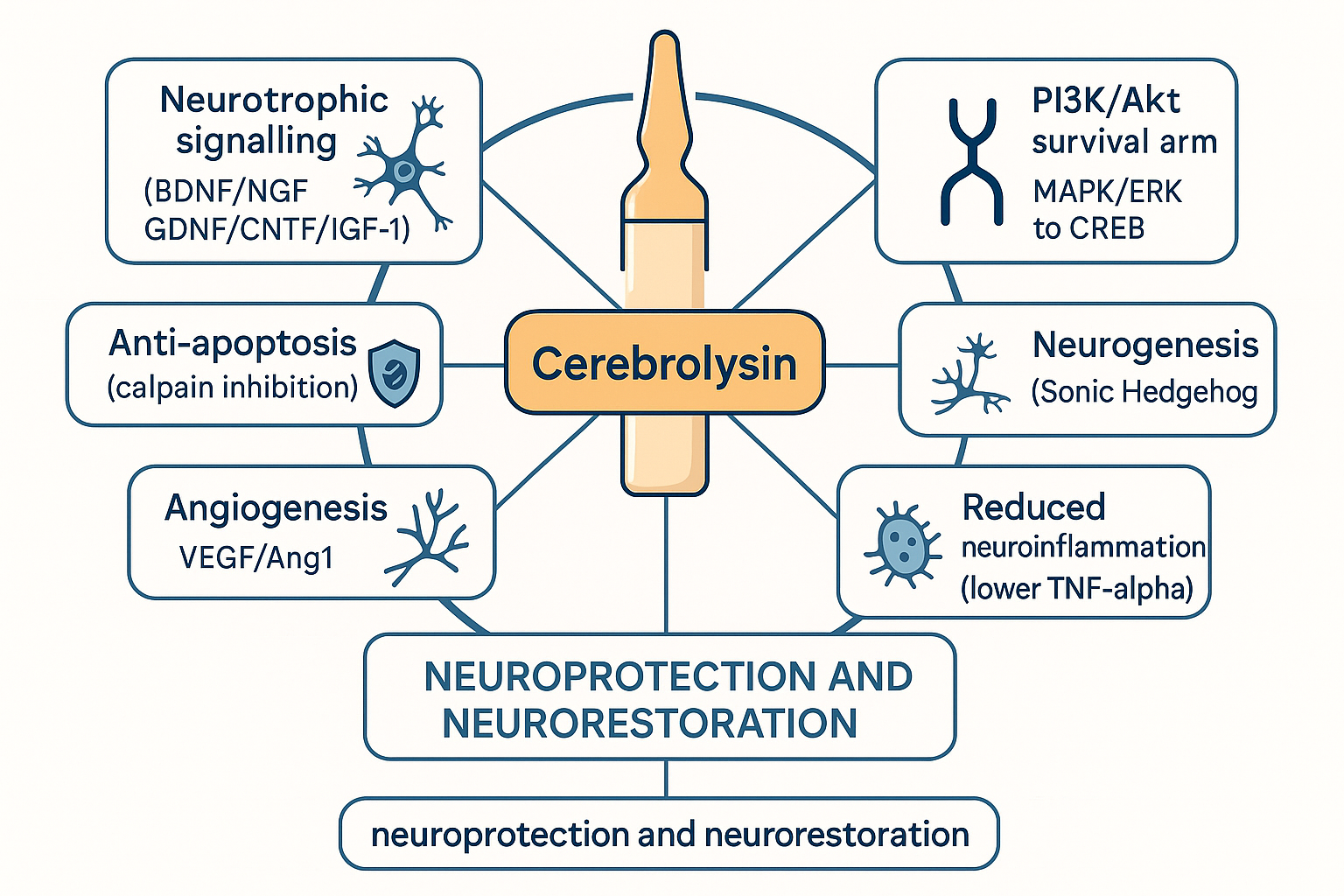 One input, many converging arms. The breadth is the selling point and the scientific problem: a drug that does ten things at once is very hard to falsify.
One input, many converging arms. The breadth is the selling point and the scientific problem: a drug that does ten things at once is very hard to falsify.
The pieces, individually:
- Calpain inhibition / anti-apoptosis. After ischaemia, calpains (calcium-activated proteases) execute neurons. Cerebrolysin inhibits calpain-mediated proteolysis and shifts the Bcl-2/Bax balance toward survival, protecting mitochondrial membranes and blocking cytochrome-c release (PeptideInsight). This is the most mechanistically solid claim.
- Excitotoxicity reduction. It dampens glutamate-driven NMDA over-activation — the same excitotoxic cascade described in the thiamine deep dive.
- Sonic Hedgehog (SHH). Beyond trophic factors, Cerebrolysin modulates SHH signalling, which drives neurogenesis in the subventricular zone and dentate gyrus and supports vascular formation — one of the few non-trophic pathways consistently named in the literature.
- Angiogenesis (VEGF/Ang1). New vessel growth into damaged tissue — the same vascular-supply logic that underpins the BPC-157 deep dive, here aimed at the brain rather than tendon and gut.
- Anti-neuroinflammation. Lowered TNF-α and modulated microglia — shifting microglia away from the chronically inflamed, neurotoxic phenotype.
⚖️ Calibration. Almost all of this mechanistic detail comes from in vitro and animal work, much of it funded or facilitated by the manufacturer, and a good deal of it now amplified by peptide-vendor blogs (cited above for convenience, not authority). The pathways are real and the biology is plausible. What "potentiates entire signalling cascades" does not tell you is how much, in whom, and whether it changes outcomes that matter. Mechanistic richness is not clinical proof — and Cerebrolysin is the clearest case in this database of those two things diverging.
Chemistry & pharmacokinetics: the active-fraction problem
Because Cerebrolysin is a mixture, its pharmacokinetics are genuinely strange and partly unknowable.
- There is no single half-life. Different peptides clear at different rates. Reported figures put the peptide mixture's plasma half-life around 2–4 hours, while the smallest/BDNF-like fragments may clear in ~10 minutes (realpeptides.co PK). Elimination is by renal filtration of the small intact peptides plus proteolytic degradation in plasma and tissue.
- A PK/PD paradox. Like BPC-157, the measured plasma persistence is short but the biological effect is described as lasting far longer — consistent with downstream signalling cascades that, once triggered, run on their own. This is the standard justification for course dosing: you don't keep a drug level up, you deliver repeated daily pulses that each kick off a multi-hour-to-multi-day signalling programme, and you stack those pulses over a 10–30 day cycle.
- The active-fraction debate. Nobody can point to the active molecule, because there probably isn't one — and that is both a feature and an embarrassment. A 2023 nanoLC-MS analysis (ScienceDirect) characterised the active peptide constituents and confirmed a complex mixture of short-chain peptides rather than any single defined entity. For a regulator used to "one drug, one mechanism, one assay," this is a nightmare; for the "whole-cascade" thesis, it's the point.
- Why oral fails. Swallow it and gut proteases plus first-pass metabolism shred the peptides before they reach circulation — the generic fate of peptide drugs, which is why it is an injectable. Morph again: "rapidly degrades when ingested, pin to win."
The clinical evidence — read this section slowly
This is where Cerebrolysin earns its place as the database's flagship calibration case. The compound is simultaneously (a) a real, approved, decades-old pharmaceutical with a plausible mechanism and (b) a drug whose best Western evidence base ranges from "weak positive" to "probably nothing." Both are true. Hold both.
Two structural facts shape everything below:
- It's approved in 50+ countries but not by the FDA or EMA. Approval in Russia/China/Eastern Europe reflects a different regulatory history and evidentiary bar, not an FDA-equivalent verdict. Absence of FDA approval here is not mere bureaucratic lag — the Western RCT base genuinely hasn't cleared the bar.
- The manufacturer funds much of the research. EVER Pharma sponsored or facilitated a large share of the pivotal trials. This doesn't make the data fraudulent, but sponsor involvement in design, randomisation, statistics and reporting is a well-documented source of inflated effect sizes — and Cochrane flagged exactly this.
flowchart LR
subgraph STRONGER["Better-supported"]
VD["Vascular dementia<br/>Cochrane: cognition + global<br/>function improved, but<br/>'not definitive'"]
TBI["Moderate–severe TBI<br/>CAPTAIN meta-analysis:<br/>'small-to-medium' benefit,<br/>n=185, manufacturer-run"]
end
subgraph MIDDLE["Mixed / suggestive"]
AD["Alzheimer's<br/>some positive signals,<br/>small trials, short follow-up"]
end
subgraph WEAKER["Null / negative"]
STROKE["Acute ischaemic stroke<br/>Cochrane ×3 editions:<br/>NO benefit on death/dependency<br/>+ ↑ non-fatal serious AEs"]
end
NOTE["Cross-cutting caveat:<br/>sponsor bias · small n ·<br/>heterogeneity · high risk of bias"]
NOTE -.-> STRONGER
NOTE -.-> MIDDLE
NOTE -.-> WEAKERAn honest evidence map. Note the inversion of community intuition: the indication biohackers cite most (stroke/brain repair) has the weakest trial support, while the quieter vascular-dementia signal is the most defensible.
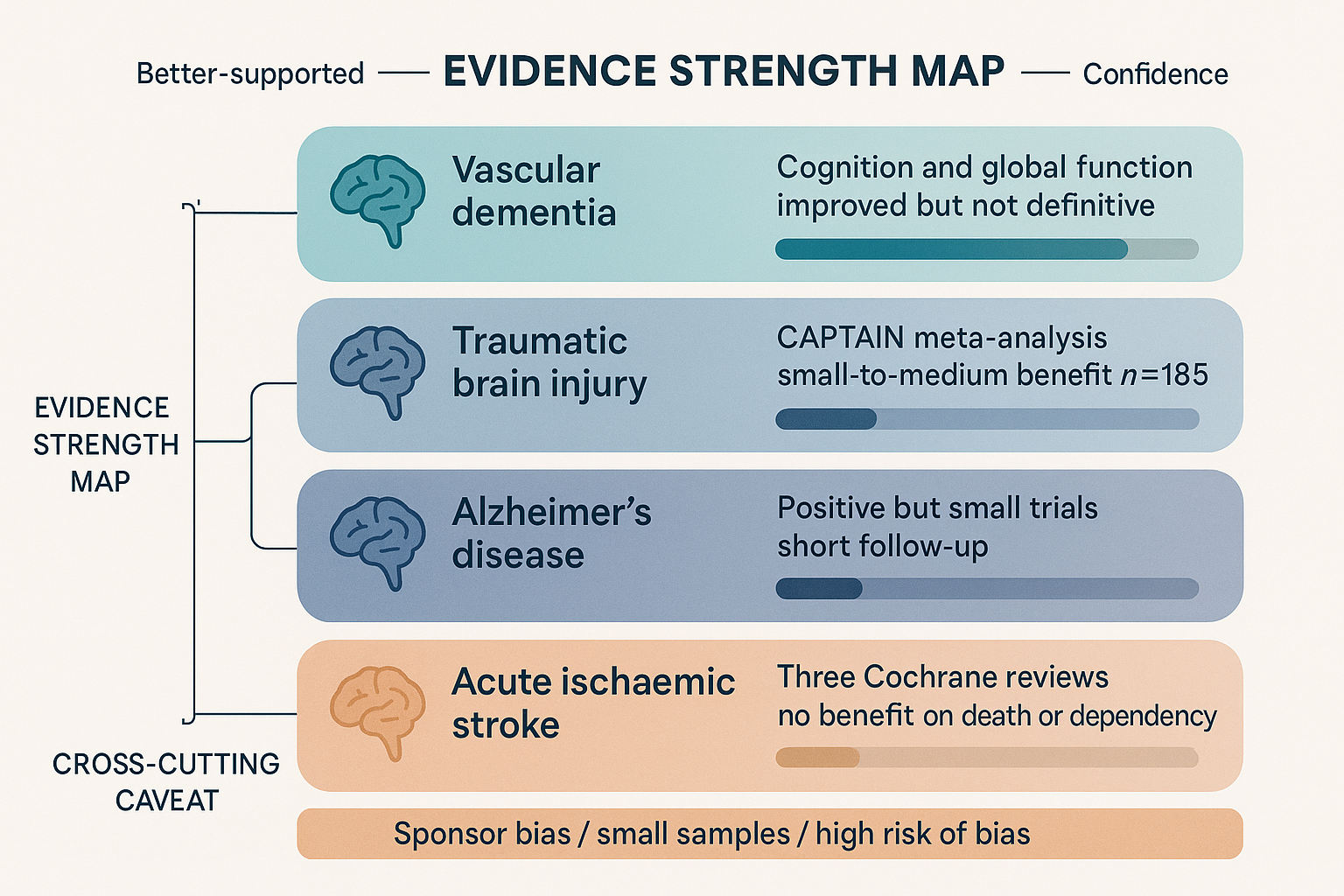 Evidence strength is not uniform across indications. The strongest signal (vascular dementia) is still rated "not definitive"; the most-hyped use (acute stroke) is where three successive Cochrane reviews found nothing.
Evidence strength is not uniform across indications. The strongest signal (vascular dementia) is still rated "not definitive"; the most-hyped use (acute stroke) is where three successive Cochrane reviews found nothing.
Acute ischaemic stroke — the Cochrane null
This is the most-tested indication and the most sobering. The Cochrane review (Ziganshina et al.), now in its third successive edition reaching the same conclusion (2010, 2020, and 2023 / pub7), pooled 7 RCTs / 1,773 participants and found:
- No evidence of benefit on all-cause death (RR 0.96, 95% CI 0.65–1.41).
- No convincing benefit on dependency/functional outcome.
- A statistically significant increase in non-fatal serious adverse events (RR 2.39, 95% CI 1.10–5.23; 3 trials, 1,335 participants).
- Overall certainty of evidence rated low to very low.
- Explicit sponsor-bias concern: three trials involved the manufacturer in design, drug provision, randomisation codes, statistics and reporting, raising the risk of bias to high.
That is about as clear a "no convincing benefit" as Cochrane issues. stinkykoala314 (@stinkykoala314) claims "Cerebrolysin can effectively treat and sometimes literally cure TBIs" — but for the closely related vascular insult of stroke, the controlled data do not support a survival or dependency benefit.
Vascular dementia — the genuine signal
Here the picture flips, and this is the strongest case for Cerebrolysin. The Cochrane review on vascular dementia (Cui et al. 2019, CD008900.pub3; 6 RCTs, ~597 participants) found that courses of IV Cerebrolysin improved cognition (MMSE / ADAS-cog+) and global clinical function, with no signal of harm. The crucial caveat in Cochrane's own words: the data are "not definitive," the trials carried high risk of bias and heterogeneity, and "if there are benefits… the effects may be too small to be clinically meaningful." So: a real, replicated, positive direction — wrapped in genuine uncertainty about magnitude.
Alzheimer's disease — suggestive, small
Multiple small RCTs report cognitive and global-function improvements in mild-to-moderate Alzheimer's, sometimes persisting weeks after the treatment course ended (consistent with the trophic/neurogenic mechanism). The literature is more positive than for stroke but limited by small samples, short follow-up and the same sponsor footprint. Promising, not settled.
Traumatic brain injury — the community's favourite, modestly supported
TBI is where biohacker enthusiasm runs hottest. The best controlled evidence is the CAPTAIN trial series — two phase IIIb/IV randomised, double-blind, placebo-controlled trials in moderate–severe TBI (GCS 6–12), using 50 mL/day for 10 days then two further 10 mL/day cycles. The prospective meta-analysis (n=185) found a "small-to-medium" effect favouring Cerebrolysin on a multidimensional functional/neuropsychological endpoint, significant at Day 30 and Day 90. Real, directionally positive, but a small, manufacturer-run dataset — not the slam-dunk "cure" the community implies.
⚖️ The calibration, in one line. Cerebrolysin's mechanism is broad and plausible; its best clinical evidence (vascular dementia) is real but rated "not definitive"; and its most-hyped indication (acute stroke) is precisely where three Cochrane reviews found no benefit and a possible safety signal. Biohacker enthusiasm has outrun the RCT base — and it has done so most in exactly the direction the trials least support.
Safety, and the prion question — addressed seriously
Cerebrolysin's acute tolerability in trials is good: the main adverse events are mild (transient agitation, sweating, dizziness, injection-site reactions), and rapid IV bolus can cause a hot/flushed sensation, which is why infusions are given slowly (over ~60 minutes) or diluted. The one non-trivial controlled safety signal is the increase in non-fatal serious adverse events in the acute-stroke Cochrane data — worth weighting, especially given that population's fragility.
The question people actually ask is about prions. It is porcine central nervous system tissue, and CNS tissue is the canonical high-risk material for transmissible spongiform encephalopathies (TSEs). This deserves a straight answer, not a dismissal:
- The substrate matters. Unlike cattle (BSE) and humans (CJD), pigs have no documented naturally-occurring prion disease. There is no known porcine TSE circulating in herds. That is the single most important fact and it materially lowers the baseline risk relative to, say, a bovine-brain product.
- The process matters. Manufacturing includes delipidation, proteolysis, filtration and purification steps that reduce (though no process guarantees elimination of) prion infectivity, and EVER Pharma sources from controlled herds under pharmaceutical TSE-risk-management requirements.
- The track record matters. The product has been in clinical use for decades across 50+ countries with no documented case of prion transmission. Morph's blunt version: "been around for 60+ years and no cases of prions yet."
Honest framing: the theoretical risk is non-zero because prions are uniquely resistant and you can never prove a negative — but the empirical risk, given a prion-free source species, TSE-managed sourcing, a purification process, and a multi-decade clean record, is very low. This is a different and more reassuring risk profile than the surface phrase "injecting pig brains" suggests.
Practical: dosing, sourcing, handling
Clinical course dosing (the evidence-based regimens): Cerebrolysin is given as courses, not continuously — daily injections for a 10–30 day cycle, often repeated. Typical clinical ranges:
| Indication | Dose | Schedule |
|---|---|---|
| Vascular dementia / AD | 10–30 mL/day IV | 10–28 days/course; courses repeated |
| Acute ischaemic stroke (trials) | 30 mL/day IV | ~10–21 days |
| Moderate–severe TBI (CAPTAIN) | 50 mL/day → 10 mL/day | 10 days, then 2 further cycles |
| General neurorecovery | 10 mL/day | 10–30 consecutive days |
IV is infused slowly (≤50 mL diluted, over ~60 min). Lower volumes (≤5 mL) are given IM.
The biohacker protocol — Bryan Johnson's is the cleanest example. Bryan Johnson (@bryan_johnson) ran Cerebrolysin as a measured, biomarker-driven longevity experiment rather than a vibe:
"Because a prior measurement indicated that I have swelling in my brain from my internal jugular vein stenosis (IJVS), we are examining the effectiveness of cerebrolysin in mitigating inflammation… Protocol: Ten, 5 mL intramuscular injections over 20 days. Cost: $160."
Note the discipline: a reason (IJVS-driven brain swelling on MRI), defined outcome measures (brain MRI markers, sleeping HRV via WHOOP, cognitive testing), and — critically — the honesty: "We cannot recommend that anyone else participates until more extensive clinical trials have been performed." That 10 × 5 mL IM over 20 days is the de-facto community starter cycle.
Community dosing skews to 1–5 mL/day IM, often every-other-day, in 10–20 day cycles. aestheticprimal (@aestheticprimal) runs "5mL Cerebrolysin (EOD)" in a dopamine-baseline stack; BasedBiohacker (@BasedBiohacker) slots "cerebrolysin 5ml (10 days)" into a 4–8 week neuroprotection block.
Sourcing. It is pharma-grade and ampouled, so the sourcing problem is access, not synthesis quality — the opposite of a research-chemical peptide. Morph: "i buy it pharma-grade from eastern europe." aestheticprimal adds region-specificity: "it's very different per region, Rupharma is decent, but even Indiamart is a better alternative." This is also the in-joke behind Morph's line that "the REAL reason Andrew Tate moved to Romania … is because it's easier to get your hands on cerebrolysin" — access tracks jurisdiction.
Handling. Supplied as a clear-to-slightly-amber aqueous solution in glass ampoules; refrigerate, protect from light, use promptly once opened, and do not mix in the same infusion with amino-acid solutions or certain other agents (manufacturer incompatibility warnings apply). Discard discoloured ampoules.
How this fits the rest of the database
Cerebrolysin is a hub compound — 16 mentions — and the way the community talks about it is itself informative.
Morph's "single greatest nootropic ever created." Morph (@doctormorphh) opens with a homage — "Can we take a second to thank Gerhart Harrer for creating this absolute pharmaceutical masterpiece?" — and a literal symptom→Cerebrolysin lookup table: "Stressed? Cerebrolysin. Brain fog? Cerebrolysin. Concussion? Cerebrolysin. Stim tolerance? Cerebrolysin… The single greatest nootropic ever created." His deep mechanistic thread is the best community articulation of the whole-cascade thesis and is worth reading in full. The honest counterweight: the "single greatest" framing is a mechanistic judgement (breadth of pathway coverage), not an outcomes judgement (RCT effect sizes) — and the gap between those two is this page's whole point.
Morph's critique of Semax sharpens the contrast. In his Semax takedown, Morph argues you "shouldnt use semax for cognition, at all," because pure BDNF-pushers are too single-target — and lists Cerebrolysin among the "TON of better shit." That's the whole-cascade-vs-single-target thesis turned into a buy recommendation. See the Semax & Selank deep dive for the other side.
The P21 connection — Cerebrolysin as a source of derivatives. nootropicguy (@nootropicguy) makes a striking claim: P21 "is a derivative of Ciliary Neurotrophic Factor (CNTF) and was developed by reverse-engineering the magic behind Cerebrolysin (Cerebrolysin is the #1 nootropic tool of all-time)." P21 is the attempt to take the defined, synthesisable, single-molecule lesson out of the undefined soup — the same trophic intent, productised into one CNTF-derived peptide. See P21. If Cerebrolysin is the whole orchestra, P21 is one instrument transcribed.
Bryan Johnson's measured longevity framing (above) is the responsible mirror image of Morph's maximalism: same compound, opposite epistemics — biomarker-gated, explicitly non-recommendation, IJVS-justified. Both belong in an honest picture.
aestheticprimal's two angles. First, glucose metabolism: in his brain-glucose thread he files Cerebrolysin alongside "actovegin, meldonium, intranasal insulin, mexidol" as compounds that "enhance brain glucose metabolism as one of their MOAs" — a bioenergetic reading that ties Cerebrolysin to Actovegin (another porcine-derived, glucose-oxidation-focused preparation) and to the thiamine energy-metabolism story. Second, dopamine baseline: in his dopamine stack he reasons Cerebrolysin lifts dopaminergic tone "mainly through improving redox balance… and also seemingly through activation of GDNF receptor complex," reporting his "Dopamine baseline seems to be much much higher." He also flags a caution worth keeping: he's "not a fan of things that rapidly induce neuroplasticity because they very often mess up top-down control from the prefrontal cortex" — and rates Pinealon and Cortexin as gentler cognition tools.
The rabbit-hole framing. BasedBiohacker (@BasedBiohacker) reduces it to a one-word answer — "procrastination? → cerebrolysin" (paired, tellingly, with "brain fog? → bpc-157 fix your gut"). The contrast with BPC-157 is instructive: BPC-157 repairs the brain indirectly via the gut-brain axis and angiogenesis; Cerebrolysin aims at the neuron directly via trophic signalling. Two routes to the same destination, which is why the community stacks them.
Where Cerebrolysin sits, then: it is the broadest-acting, best-credentialled, hardest-to-source entry in the brain-repair cluster — a real pharmaceutical that the biohacking world has elevated above what its Western trial data can carry.
Bottom line
Cerebrolysin is the most interesting honesty test in this database. The mechanism is genuinely attractive: a standardised peptide hydrolysate that sidesteps the blood-brain-barrier wall that killed every recombinant neurotrophic-factor drug, and that plausibly nudges the entire trophic/vascular/anti-apoptotic/neurogenic/anti-inflammatory network rather than one node. It is a real, approved, decades-old drug with a clean prion record from a prion-free source species. The community reverence — Morph's "single greatest nootropic ever created," nootropicguy's "#1 of all-time" — is built on something real.
And yet: three successive Cochrane reviews find no convincing benefit in acute stroke and a possible safety signal; the genuinely positive indication (vascular dementia) is rated by Cochrane itself as "not definitive," with effects that "may be too small to be clinically meaningful"; the TBI evidence is a small, manufacturer-run, "small-to-medium" effect; and sponsor bias shadows the entire literature. The FDA's and EMA's non-approval is not just lag.
The defensible position is neither "miracle" nor "dismiss." It is: a mechanistically rich, broadly-acting, well-tolerated neurorestorative whose Western RCT base is thin, sponsor-shadowed, and most absent precisely where enthusiasm is loudest. If you use it, do it the Bryan Johnson way — a defined reason, defined outcome measures, a bounded course — not the symptom-lookup-table way. The biology earns curiosity. The data do not yet earn the certainty the timeline gives it.
Research sources
Composition / manufacturing - Active-peptide identification by nanoLC-MS (mixture, not single entity): ScienceDirect / J Chromatogr B (2023) - Cerebrolysin overview (composition, EVER Pharma): ScienceDirect Topics - Porcine-derived neuropeptide guide (75% amino acids / 25% peptides <10 kDa): superpower.com
Mechanism - Mechanism overview (Trk, PI3K/Akt, MAPK/ERK/CREB, SHH, endogenous BDNF/VEGF/IGF-1, ↓TNF-α): realpeptides.co - Anti-apoptotic / Bcl-2-Bax / calpain detail: PeptideInsight
Clinical evidence - Acute ischaemic stroke — Cochrane 2023 (pub7), Ziganshina et al. (no benefit on death/dependency; ↑ non-fatal serious AEs; sponsor bias): Cochrane Library CD007026.pub7 · 2020 pub6 · PMC10565895 - Vascular dementia — Cochrane 2019 (CD008900.pub3), Cui et al. (cognition + global function improved; "not definitive"): Cochrane Library · PubMed 23440834 - TBI — CAPTAIN prospective meta-analysis (moderate–severe TBI, n=185, "small-to-medium" benefit): PubMed 33620612 · Springer / Neurol Sci
Pharmacokinetics - Half-life / elimination / PK-PD paradox: realpeptides.co
Safety / prions - Prion-risk assessment (prion-free source species, process controls, no transmission cases): PeptideInsight · Project BioHacked
Manufacturer mechanism-of-action booklets (sponsor material — read critically): cerebrolysin.com MoA booklet; cited by Morph's thread.
All community quotes compiled from biohacking Twitter/X discussions. Educational purposes only. Not medical advice. Cerebrolysin is an injectable prescription drug in the countries where it is approved, and is not approved by the FDA or EMA. Several cited vendor/peptide blogs are commercial sources included for convenience, not as primary evidence — weight the peer-reviewed Cochrane and trial citations accordingly.