Cavities, Dental Health & the Mouth-Gut Axis
Why the "drill and fill" model treats the hole and ignores the disease, why teeth can actually remineralise, what mastic gum really does to the bacteria your toothbrush can't reach, and how the health of your mouth and the health of your gut are two ends of one continuous tube.
Read alongside
The mouth is the first segment of the digestive tract, so this page sits directly on top of three foundations: Digestion (the mouth as stop one), the Gut Microbiome (the oral microbiome seeds and mirrors the gut one), and Inflammation (gum disease is chronic inflammation with body-wide reach).
Why this page exists
A cavity, in the conventional telling, is a mechanical problem: a hole in a tooth that a dentist drills clean and fills. This page argues — following a cluster of well-sourced threads from the biohacking world (Healthy Alfred, Dalton/@Outdoctrination, Veronica/@celestialbe1ng, @OnlyThroughGod) — that this view is half the story, and the missing half explains both why cavities keep coming back and how they can sometimes be prevented or even reversed without a drill.
The deeper picture has three parts that the rest of this page builds out:
- A cavity is a bacterial disease, and filling the hole leaves the bacteria alive — which is where the antimicrobial angle (mastic gum, biofilms) comes in.
- A tooth is a living, dynamic tissue in constant flux between dissolving and rebuilding — which is where remineralisation, hydroxyapatite, and the fat-soluble vitamins come in.
- The mouth is the entrance to the gut, so oral and gut health are mechanically and microbially linked — which is the part the user most wants, and the part conventional dentistry ignores entirely.
We take them in turn. As always, claims that run ahead of the evidence are flagged ⚖️ Calibration.
What a cavity actually is
A tooth's hard outer shell is enamel — the hardest substance in your body — and beneath it dentin. Both are built largely from a calcium-phosphate mineral called hydroxyapatite (remember that word; it returns). A cavity (dental caries) is, at root, the dissolving of that mineral by acid.
Where does the acid come from? Bacteria. Specifically Streptococcus mutans (S. mutans), the organism Healthy Alfred correctly calls "the #1 cause of cavities." The sequence:
- S. mutans colonises the tooth surface and feeds on dietary sugar.
- As it ferments that sugar, it excretes acid (lactic acid).
- The acid dissolves the hydroxyapatite mineral out of the enamel — demineralisation — layer by layer.
- Left unchecked, the demineralised spot deepens into a hole: a cavity.
So a cavity is not really "a hole" — the hole is the end result. The actual disease is an acid-producing bacterial colony fed by sugar. This reframes the standard treatment exactly as Alfred puts it: "your dentist drills it out, fills the hole… the bacteria? still alive." Drilling and filling repairs the damage but does nothing about the cause — which is why people who get one filling so often get more.
The biofilm problem: why brushing and mouthwash fall short
Here is the part that surprises people. S. mutans doesn't float around loose — it lives inside a biofilm, the sticky, structured bacterial community you know as dental plaque. A biofilm is not a smear of germs; it's an organised fortress: the bacteria embed themselves in a self-made matrix that shields them from the outside, including from antimicrobials and from your immune cells. (This is the same biofilm concept from the gut microbiome page, applied to the tooth.)
The consequence, in Alfred's framing: "your toothbrush scrubs the surface. your mouthwash splashes the top. neither touches the colony underneath." Brushing mechanically removes the outer layer of plaque (genuinely useful — it keeps the biofilm thin), and mouthwash kills surface bacteria, but neither reliably penetrates the deeper biofilm or the subgingival (below-the-gumline) pockets where the worst organisms hide. Dental hygienists spend careers scraping that subgingival layer off with scalers precisely because nothing topical reaches it well.
This is the gap the mastic gum claim aims at.
Mastic gum: the antimicrobial angle
Mastic gum is a resin from the Pistacia lentiscus tree (the Greek island of Chios), chewed for thousands of years. Its relevant chemistry: it contains triterpenoids (and related acids) that are antimicrobial and — the key claim — lipophilic enough to penetrate the biofilm that toothbrushes and mouthwashes can't. The threads cite a specific body of evidence:
- PMID 16343417 (Aksoy et al., Archives of Oral Biology, 2006) — mastic chewing gum significantly reduced S. mutans counts in human saliva (the "p<0.001" Alfred quotes) and reduced plaque.
- PMID 16822220 — activity against Porphyromonas gingivalis (P. gingivalis), a major gum-disease (periodontitis) pathogen.
- PMID 9874617 (Huwez et al., New England Journal of Medicine, 1998) — mastic gum activity against Helicobacter pylori (H. pylori) — and this one is the bridge to the gut, because H. pylori is a stomach pathogen, not an oral one (more below).
The proposed mechanism, as Alfred relays it: the triterpenoids penetrate the subgingival biofilm, rupture bacterial cell walls, and block replication — reaching "chemically, between appointments" the layer a hygienist can only reach mechanically. And because it's a broad physical/chemical attack rather than a single molecular target, the claim is "zero resistance in 3,000 years" (plausible for this kind of mechanism, though "zero" is rhetorical).
The protocol Alfred gives in the replies: chew after meals, 2–3 times daily, 1–2 g total, consistency over dose, ~4–6 weeks to notice an oral-health shift.
⚖️ Calibration. The in-vitro and small-trial evidence that mastic gum lowers S. mutans and plaque is real and reasonably consistent. But note the scale: these are mostly small or short studies, not large RCTs showing fewer cavities over years. The famous NEJM H. pylori result (1998) was a small study, and later eradication trials were more mixed — mastic likely suppresses H. pylori rather than reliably eradicating it. So: a credible, low-risk antimicrobial adjunct that targets the real cause (the bacteria), not a proven replacement for brushing, flossing, or a dentist. "Kills it" is stronger than "suppresses and reduces," which is what the data actually support.
Teeth are alive: the remineralisation model
Now the second big idea, the one that makes "reversing cavities" even conceivable. Most people imagine teeth as inert stones. They are not. Enamel is in constant two-way exchange with the saliva bathing it:
- Demineralisation — acid pulls calcium and phosphate out of the enamel (the cavity process above).
- Remineralisation — when conditions are right, calcium and phosphate from saliva are deposited back into the enamel, rebuilding the mineral.
Your teeth are demineralising and remineralising all day long. A cavity forms only when the balance tips toward dissolving for long enough. This means an early lesion — demineralised but not yet a physical hole — can be pushed back the other way and re-hardened. (An already-cavitated, collapsed hole in dentin generally cannot fully regrow and still needs a filling — an important limit, see calibration.)
What governs which way the balance tips:
- Saliva — your natural remineralising fluid, carrying calcium, phosphate, and buffering agents. Anything that improves saliva flow and quality (including, per the vitamin D data below) protects teeth.
- Acid exposure / sugar frequency — every sugar hit feeds S. mutans and tips toward demineralisation. Frequency matters more than amount: constant grazing keeps the mouth acidic.
- The mineral supply — whether the raw materials (calcium, phosphate) and the signals to deposit them are present.
This is where hydroxyapatite toothpaste enters. Rather than the fluoride approach (which makes enamel more acid-resistant by forming fluorapatite), hydroxyapatite toothpaste supplies the actual mineral the tooth is made of, providing calcium-phosphate building blocks directly to remineralise the surface. It's the mineral-replacement strategy, and it's non-toxic if swallowed — which is why the biohacking world (and @OnlyThroughGod's cavity-reversal anecdote) favours it.
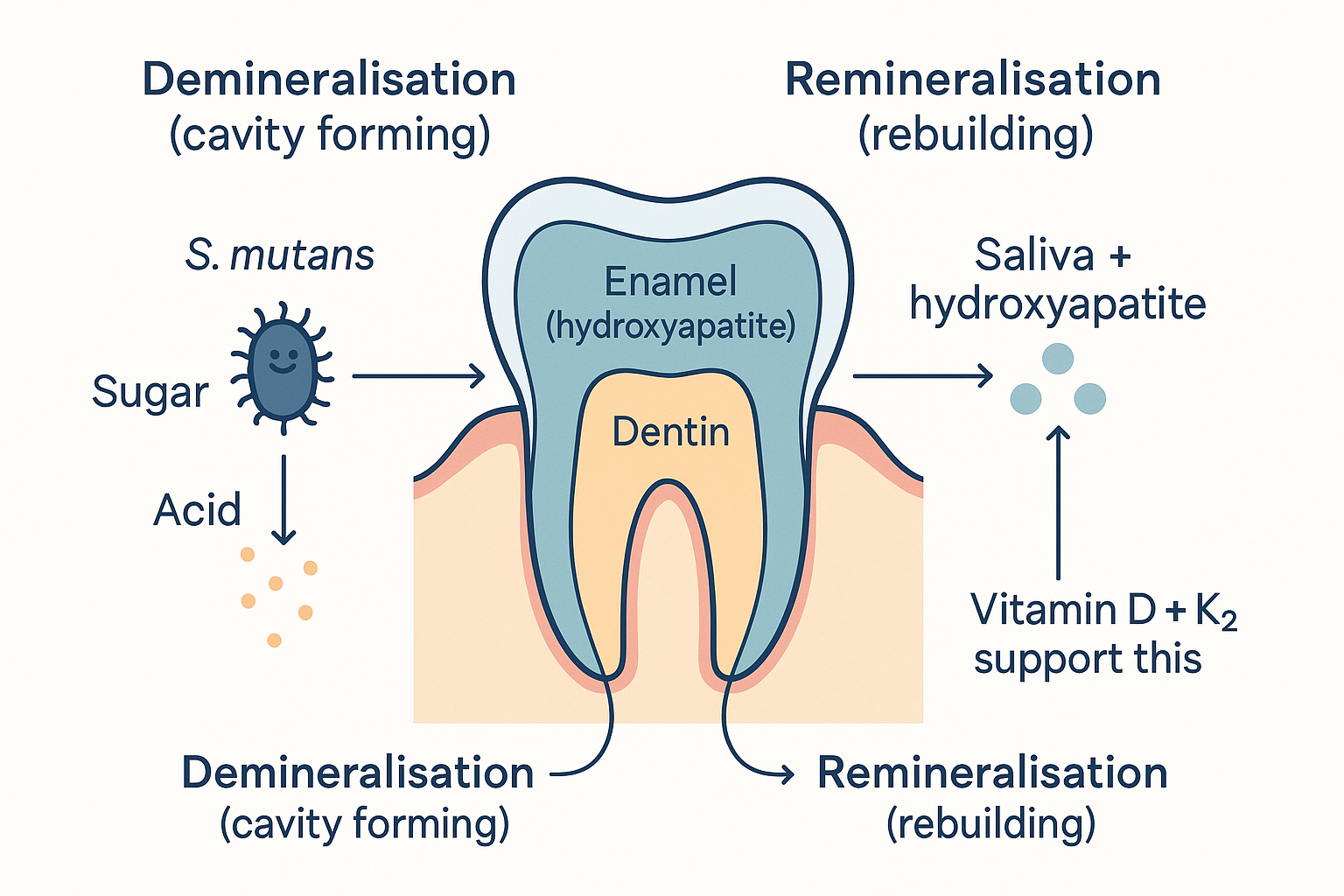 A tooth is in constant two-way exchange: acid from sugar-fed bacteria pulls mineral out, while saliva, hydroxyapatite, and the fat-soluble vitamins put it back. A cavity is just this balance tipped toward dissolving.
A tooth is in constant two-way exchange: acid from sugar-fed bacteria pulls mineral out, while saliva, hydroxyapatite, and the fat-soluble vitamins put it back. A cavity is just this balance tipped toward dissolving.
flowchart LR
subgraph DEMIN["DEMINERALISATION (cavity forming)"]
SUGAR[Sugar / frequent acid] --> SM[S. mutans makes acid]
SM --> DISS[Mineral dissolves out of enamel]
end
subgraph REMIN["REMINERALISATION (tooth rebuilding)"]
SALIVA[Saliva + calcium/phosphate] --> DEP[Mineral deposited back]
HAP[Hydroxyapatite toothpaste] --> DEP
SIGNAL["Vitamin D + K2 signals<br/>(see below)"] --> DEP
end
DISS <-->|"the daily balance —<br/>a cavity is just this tipped<br/>toward dissolving"| DEPThe systemic angle: cavities as a nutritional disease
The third idea is the oldest and most radical: that whether your teeth remineralise is largely decided by your nutrition, not just your brushing — that dental caries is, in part, a systemic, nutritional disease. This is the Weston Price tradition (a 1930s dentist who linked traditional fat-soluble-vitamin-rich diets to cavity-free populations), and the threads marshal real evidence for it.
The key nutrients, drawn from Dalton's "8 nutrients for dental health" thread and Veronica's K2 thread:
Vitamin D — the master signal
Vitamin D does several distinct things for teeth, which is why Dalton leads with it:
- Promotes calcium absorption — no vitamin D, no calcium uptake, no mineral to deposit (the digestion and liver link: D is a fat-soluble vitamin needing gut + liver to activate).
- Drives production of antimicrobial peptides (like cathelicidin) in the mouth — your own built-in antibiotics that suppress S. mutans and plaque.
- Promotes saliva secretion — more remineralising fluid.
- Directly supports enamel and dentin formation — vitamin D deficiency shows up as enamel hypoplasia (defective, pitted enamel — the "Figure 3" in Dalton's thread).
The cited data: saliva from people taking 1,000 IU vitamin D/day remineralised acid-dipped teeth and nearly restored their hardness (Vickers hardness testing), and a systematic review found vitamin D supplementation cut cavity risk by roughly 50% (this is the Hujoel 2013 analysis). Optimal blood level cited: >40 ng/mL (>100 nmol/L), with sunlight as the primary source.
Vitamin K2 — the calcium traffic director
If vitamin D gets calcium into the blood, vitamin K2 decides where it goes — and you want it in teeth and bone, not arteries. K2 activates two proteins (osteocalcin and matrix Gla protein) that bind calcium into the hard tissues. Dalton's thread shows K2 status is inversely related to gum inflammation, plaque, bleeding, and tooth-pocket depth — i.e. lower K2, worse periodontal disease. Veronica's thread adds the historical hook: a 1946 Northwestern University study found a vitamin-K + calcium chewing gum reduced new cavities by 60–90%, and notes people swishing K2 MK-4 directly on teeth with good results. The dietary sources are the "whole milk propaganda" she half-jokes about — K2 is rich in full-fat dairy, butter from grass-fed cows, egg yolks, and natto.
The supporting cast
- Calcium and phosphorus — the literal mineral building blocks of hydroxyapatite.
- Magnesium — required to use calcium and vitamin D properly (the magnesium deep dive).
- Vitamin A — for healthy enamel-forming cells and mucosal/saliva integrity.
- Vitamin C — for the collagen of gums and dentin (scurvy is, classically, a gum disease).
The unifying claim: give the body the fat-soluble vitamins (A, D, K2) plus the minerals, and the remineralisation machinery has both the materials (calcium/phosphate) and the signals (D and K2) to keep the daily balance tilted toward rebuilding.
⚖️ Calibration. The vitamin D → caries reduction evidence is genuinely good (multiple studies, a coherent mechanism). The K2 evidence is more associative (the inverse correlations are real; the 1946 gum study is old, small, and industry-linked — treat the "60–90%" as a historical curiosity, not a modern endpoint). The big honest limit on the whole "reverse cavities" theme: nutrition and hydroxyapatite can remineralise early, non-cavitated lesions ("white spots") and harden enamel — but a tooth with an actual collapsed hole in the dentin will not regrow that structure and still needs a dentist. The systemic model is a powerful prevention and early-reversal framework, not a cure for established cavities. Anecdotes of "the cavity was gone at follow-up" most plausibly describe early lesions that remineralised (or were borderline calls), not large holes that filled themselves in.
The mouth-gut axis: two ends of one tube
Now the connection the user specifically asked about — and it is far more than a metaphor, because the mouth is literally the first segment of the gut. From the digestion page, the digestive tract is one continuous tube from mouth to colon; the mouth is stop one. That single anatomical fact drives several real links, running in both directions:
Mouth → gut:
- The oral microbiome seeds the gut microbiome. You swallow ~1–1.5 litres of saliva a day, carrying billions of oral bacteria into the gut. A healthy, balanced oral microbiome contributes a healthy input; a dysbiotic, pathogen-heavy mouth (lots of P. gingivalis and friends) sends those organisms downstream. Periodontal pathogens have been found translocating to and colonising the gut, where they can promote gut dysbiosis and inflammation.
- Gum disease is a source of systemic inflammation. Periodontitis is a chronic inflammatory infection with an open, ulcerated surface — a continuous portal through which oral bacteria and their endotoxin (LPS) enter the bloodstream. This is why periodontal disease is statistically tied to heart disease, diabetes, and other systemic conditions: it's a chronic inflammatory and endotoxin load, exactly the kind the gut microbiome page describes leaking from a damaged barrier — but here the leak is in the mouth.
- The H. pylori bridge — the mastic gum / H. pylori finding (PMID 9874617) is a concrete mouth-to-stomach link: a tool aimed at oral bacteria also hits a stomach/gut pathogen (H. pylori causes ulcers and gastritis, and the mouth can be a reservoir for re-infection).
- Digestion starts in the mouth. Chewing and salivary enzymes (amylase) are the first step of digestion; poor dentition and poor chewing mean larger food particles and more downstream digestive burden.
Gut → mouth:
- The gut decides whether the dental nutrients are absorbed. The remineralisation vitamins (A, D, K2) are all fat-soluble, so they depend on good gut absorption, bile, and a healthy gut barrier (digestion and liver pages). A compromised gut → poor fat-soluble-vitamin status → teeth that can't remineralise. So "fix your teeth" can require "fix your gut" first.
- Some gut bacteria make K2. Gut bacteria synthesise some of the vitamin K that supports the calcium-directing machinery — another way gut health feeds tooth health.
flowchart TD
MOUTH[MOUTH<br/>oral microbiome, plaque, gums] -->|"swallowed saliva<br/>seeds the gut"| GUT[GUT<br/>microbiome]
MOUTH -->|"gum disease → LPS + bacteria<br/>into bloodstream"| INFLAM[Systemic inflammation]
MOUTH -->|"chewing + amylase<br/>= digestion step 1"| GUT
GUT -->|"absorbs fat-soluble<br/>vitamins A, D, K2"| REMIN[Tooth remineralisation]
GUT -->|"gut bacteria make<br/>some vitamin K2"| REMIN
REMIN --> MOUTH
INFLAM -->|worsens| GUTThe takeaway: the mouth and the gut are one ecosystem viewed at two points. A clean, well-mineralised, low-inflammation mouth sends better inputs downstream and reflects a body absorbing its fat-soluble vitamins; a dysbiotic, inflamed mouth both signals and worsens systemic and gut problems. You cannot fully separate "dental health" from "gut health" — they share a tube, a microbiome continuum, and a dependence on the same fat-soluble nutrients.
Practical synthesis: what the threads actually recommend
Pulling all four sources into a coherent protocol, organised by the three mechanisms:
1. Kill / suppress the bacteria (the antimicrobial layer):
- Mastic gum — chew after meals, 2–3×/day, ~1–2 g, consistently for 4–6 weeks. Penetrates biofilm in a way brushing/mouthwash don't; also targets gum (P. gingivalis) and stomach (H. pylori) pathogens.
- Keep mechanically removing plaque — brushing and flossing still matter (they keep the biofilm thin so the chemistry can work). The threads add to, not replace, hygiene basics.
- Cut sugar frequency — starve S. mutans; grazing is worse than a single dose.
2. Remineralise (the mineral layer):
- Hydroxyapatite toothpaste — supplies the tooth's own mineral directly; the non-toxic remineralising agent.
- Support saliva — hydration, nasal breathing, and vitamin D all help.
3. Supply the systemic nutrients (the signalling layer):
- Vitamin D — sunlight first; aim for replete status (the threads cite >40 ng/mL). Drives absorption, antimicrobial peptides, saliva, and enamel.
- Vitamin K2 (MK-4) — from full-fat dairy, egg yolk, natto, or supplement; directs calcium into teeth (some swish MK-4 directly).
- Calcium, magnesium, vitamin A, vitamin C — the supporting minerals and vitamins.
4. Fix the gut (the absorption layer):
- Because the dental nutrients are fat-soluble and gut-absorbed, a healthy gut barrier and microbiome is upstream of all of it — the same "heal the gut" theme that runs through the whole Foundations series.
⚖️ Calibration — the honest bottom line. This is a strong prevention and early-reversal framework, and every layer has a defensible mechanism. But hold three caveats: (1) an established, cavitated hole still needs a dentist — don't skip real dental care hoping to remineralise a deep cavity; (2) the antimicrobial and K2 claims rest on smaller studies than the vitamin D ones; (3) "your dentist won't tell you / has no clue" is rhetorical — good dentists do know about remineralisation, hydroxyapatite, and diet. The genuinely valuable, evidence-backed core: cavities are a sugar-fed bacterial-and-mineral-balance disease, teeth can remineralise early lesions, fat-soluble vitamins materially affect that balance, and the mouth is continuous with the gut — so treat them as one system, alongside (not instead of) conventional dental care.
Related compounds & foundations
Antimicrobial / biofilm
- Mastic gum — biofilm-penetrating antimicrobial; targets S. mutans, P. gingivalis, and H. pylori.
- Lactoferrin — an antimicrobial protein in saliva that helps control oral (and gut) bacteria; see the Lactoferrin & Colostrum deep dive.
Remineralisation
- Hydroxyapatite — the tooth's own mineral, supplied topically.
- Calcium, magnesium — the mineral building blocks and their cofactor.
Systemic signals
- Vitamin D — absorption, antimicrobial peptides, saliva, enamel.
- Vitamin K2 / vitamin K — directs calcium into teeth and bone.
- Vitamin C — gum and dentin collagen.
Related foundations
- Digestion — the mouth as stop one of the gut; fat-soluble vitamin absorption.
- Gut Microbiome — biofilms, dysbiosis, and the oral-gut microbial continuum.
- Inflammation — gum disease as a chronic systemic inflammatory load.
- Liver — activation of vitamin D and bile for fat-soluble vitamin absorption.
Sources: threads by @HealthyAlfred (mastic gum, with replies citing PMIDs 16343417, 16822220, 9874617), @Outdoctrination (8 nutrients for dental health), @celestialbe1ng (vitamin K2 + calcium, 1946 Northwestern gum study), and @OnlyThroughGod (vitamin D+K + hydroxyapatite cavity-reversal account). Referenced research: Aksoy et al. 2006 (mastic vs S. mutans), Huwez et al. NEJM 1998 (mastic vs H. pylori), Hujoel 2013 (vitamin D and caries). Mechanistic claims reflect standard cariology; therapeutic and reversal claims are flagged where they rest on smaller or older evidence.